Cardiac MRI > Pathology > Coronary Artery Disease > Acute and Chronic Myocardial Infarction
Detection and Assessment of Acute and Chronic Myocardial Infarction
![]()
The presence and extent of a myocardial infarction can be assessed with delayed enhanced imaging. Delayed hyperenhancement (DHE) is caused by delayed washout of contrast agent from the myocardium. In normal myocardium, contrast media quickly washes in and out of the myocardial interstitium. Abnomal myocardium, however, retains contrast agent which is demonstrated as enhancement on delayed imaging.
Delayed enhanced imaging is performed 10-15 minutes after the intravenous administration of 0.15-0.2 mmol/kg of gadolinium contrast media. An inversion recovery sequence is used in which normal myocardium is nulled to accentuate the delayed enhancement.
Delayed hyperenhancement may be seen in chronic infarcts as well as acute. In chronic infarcts, delayed washout is a result of scar tissue retaining contrast media. In acute infarcts, delayed washout is due to an increase in the volume of distribution of the interstitium due to destruction of myocytes and resultant edema.
Both acute and chronic myocardial infarctions will demonstrate wall motion abnormalities in the regions of infarction. Acute infarction may show increased signal on T2-weighted imaging due to edema. In severe acute infarctions, a non-enhancing area of subendocardium may be present surrounded by an area of enhancement. This pattern represents microvascular obstruction (MO) in which the ischemia is severe enough to necrose blood vessels as well as myocytes. As a result of necrotic blood vessels, contrast media is never able to reach this area. This finding usually resolves by 2 weeks, leaving only an area of DHE. The presence of MO on delayed enhanced images is indicative of a poor clinical prognosis.
The normal evolution of a myocardial infarction is progressive thinning of the myocardium in the region of the infarction with hypertophy of the non-infarcted myocardium as well as ventricular dilation. Ventricular thrombus may form adjacent to akinetic myocardium after infarction. Thrombus does not enhance on delayed enhanced images and is within the left ventricle which separates it from MO, which involves the subepicardium.
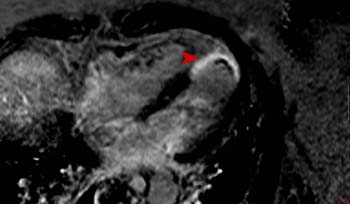
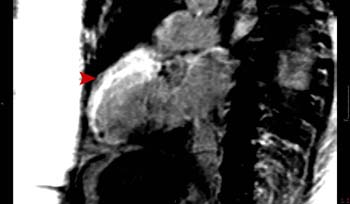
Transmural infarction of the anterior wall, apical septum, and apex. SSFP cines demonstrate akinesis of the infarcted area. Delayed enhanced images demonstrated transmural enhancement of the anterior wall, apical septum and apex resulting from a left anterior descending coronary artery occlusion. Notice the thin rim of unenhancing tissue on the 4 chamber delayed enhanced image which represents left ventricular thrombus adherent to the akinetic myocardium.
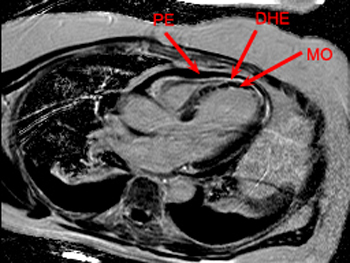
LAD territory infarction with large area of microvascular obstruction (MO). The SSFP cines shows akinesis of the apical septum and apex. The delayed hyperenhancement (DHE) image shows a large area of MO in the subendocardium. There is enhancement of the surrounding myocardium extending to the subepicardium. There is also a pericardial effusion (PE) which is black on DHE images. MO can be differentiated from thrombus by comparing the thickness of the myocardium on the SSFP images with that of the DHE images, thereby locating the unenhancing tissue of MO in the subendocardium.
Revascularization procedures such a coronary artery bypass grafting (CABG) and percutaneous transluminal angioplasty (PTA) can be used to restore blood flow to the myocardium in the setting of chronic ischemia. However, before these procedures are done, it is important to determine if the myocardium has any viable myoctyes remaining or if the area is entirely infarcted and scarred.
Regions in which there is abnormal wall motion in a coronary distribution at rest without DHE represent hibernating myocardium and are most likely to recover function after revascularization. Regions with wall motion and DHE ranging from 1% - 25% transmural thickness are likely to regain function after revascularization. Regions with 25% - 50% transmural DHE may recover function. Regions with 50% - 100% transmural DHE are unlikely to recover function.
![]()
![]()