GI Radiology > Colon > Neoplasms > Colorectal Adenocarcinoma
Neoplasms
![]()
Colorectal Adenocarcinoma |
|
|
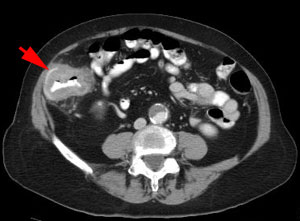
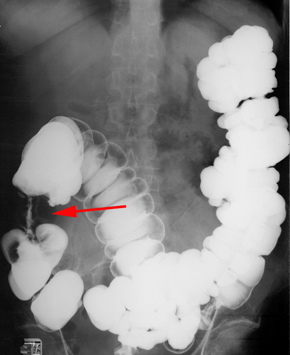
Colorectal Adenocarcinoma is the most common GI malignancy and is the second most deadly cancer in the United States. Risk factors include increasing age, personal and family history of cancer, high-fat low-fiber diet, and IBD. Signs and symptoms depend on the location of the tumor. Proximal tumors will cause occult fecal blood and anemia, whereas distal tumors will cause more changes in bowel habits and hematochezia. Approximately 50% of these malignancies develop in the rectosigmoid area and 25% in the cecum and ascending colon. Many likely arise from a malignant transformation of an adenomatous polyp. These tumors tend to form annular constricting lesions or bulky exophytic masses, with raised everted edges and ulcerated mucosa, ranging from 2-6cm in diameter. They spread by direct invasion into the pericolonic fat and adjacent organs, through lymphatic vessels to regional nodes, and hematogenously via systemic and portal circulation. Barium enemas, CT colonography, transrectal ultrasound, and colonoscopy (allows for biopsies) are the best ways to detect colorectal carcinomas. Apple-core constricting lesions, tumor masses, nodal involvement, and metastases may be visualized. A chest x-ray should also be taken to check for metastases. Staging of colon cancer is extremely important because it predicts long-term survival outcomes and helps determine whether adjuvant therapy should be given. Treatment consists of tumor resection if possible, lymph node dissection, chemotherapy and/or radiation.
CT showing cecal cancer (arrow) Apple core lesion in ascending colon (arrow) Mucinous Colon Cancer on CT (arrow) |