|
Untreated thoracic
esophageal perforations have a near 100% mortality rate because of the
fulminant mediastinitis that occurs afterwards. Perforation of the cervical
esophagus is more common and has a lower mortality rate, 15%. In either
case, early detection is important in order for prompt surgical intervention.
Perforation can be due to iatrogenic causes (i.e. endoscopic procedures,
pneumatic dilatation balloons, nasogastric tubes, endotracheal tubes),
foreign bodies, trauma, or spontaneously (Boerhaave's syndrome-see next
section).
Clinical
Cervical perforation often occurs as a complication of endoscopy. Patients
may present with dysphagia, neck pain, fever, or subcutaneous emphysema
in the neck. Cervical esophageal perforations heal with conservative treatment
with antibiotics, but larger perforations may require cervical mediastinotomy
with open drainage to prevent abscess formation.
Radiological findings
On plain films, subcutaneous emphysema may be visible on AP or lateral
films of the neck. Air may also dissect into the chest and produce a pneumomediastinum.
Lateral films of the neck may reveal widening of the prevertebral space,
anterior deviation of the trachea, or a retropharyngeal abscess with an
air-fluid level. If a cervical perforation is suspected on plain film,
the study should be followed up with a water-soluble contrast study.
Water-soluble contrasts are rapidly absorbed from the mediastinum, whereas
barium has been shown to excite an inflammatory response with fibrosis.
However water-soluble contrasts may miss 15 to 25% of perforations because
they are less radiopaque than barium. On the esophogram, one would look
for localized extravasation of contrast medium into the neck or mediastinum.
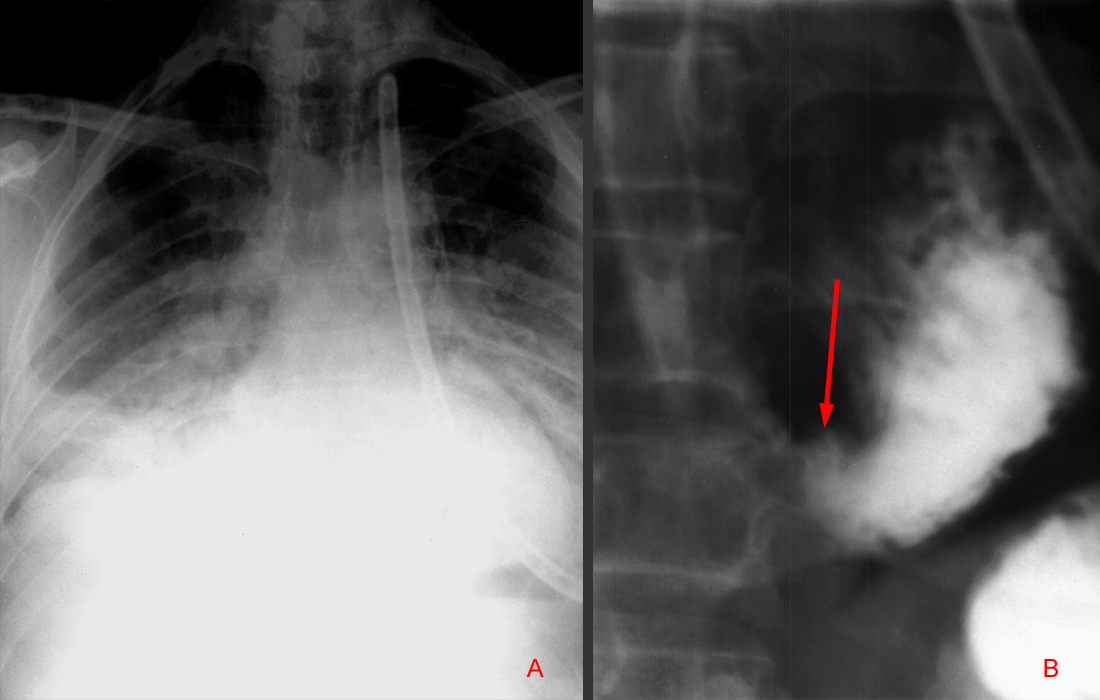
In
image "A", this frontal view of the chest shows evidence of
mediastinal and subcutaneous emphysema with pneumonitis. Image "B"
reveals an esophagram with extravasation of contrast from the esophagus.
Clinical
Thoracic perforation often present with the classic triad of vomiting,
lower thoracic chest pain and subcutaneous emphysema. Refluxed stomach
acid or swallowed food/saliva may enter the mediastinum and cause severe
mediastinitis. If no subcutaneous emphysema is present, thoracic esophageal
perforations are often mistaken as perforated peptic ulcers, MI, spontaneous
pneumothorax, pancreatitis, dissecting aortic aneurysm, or mesenteric
infarction. After 24 hours, the mortality rate for thoracic perforation
approaches 70%. Unlike cervical perforations, thoracic perforations are
treated immediately with surgery and drainage.
Radiological findings
On plain films, a widened mediastinum and pneumomediastinum may be present.
Also, approximately 75% of thoracic esophageal perforations are associated
with a pleural effusion or hydropneumothorax. Left pleural effusions often
occur because of irritation of the adjacent parietal pleura and pulmonary
parenchyma. Hydropneumothorax can occur if the mediastinal pleura ruptures
and gas and fluid may enter the pleural space directly from the mediastinum.
On esophagram, contrast media is usually seen extravasating from the left
lateral aspect of the distal esophagus because most thoracic perforations
occur near the gastroesophageal junction.
|