GI Radiology > Peritoneum > Air > Pneumoperitoneum
Pneumoperitoneum
![]()
|
Clinical Pneumoperitoneum refers simply to air within the peritoneal cavity. There are many possible causes of pneumoperitoneum including bowel perforation (most often due to perforated duodenal or gastric ulcers), trauma, recent surgery, laparoscopy, or infection of the peritoneal cavity by gas producing organisms. If the free air is due to recent surgical procedure it should resolve within 3-7 days and serial films should show decreasing amounts of free air. If the pneumoperitoneum is secondary to any of the other above causes it is a surgical emergency and should be evaluated immediately.
Radiological findings Free air on plain films is best demonstrated with a patient in the upright position. In fact, upright chest films are the most sensitive for demonstrating free air where it can be seen below the domes of the diaphragm. Several findings are characteristic of pneumopertioneum including: a) double wall sign (Rigler's) which shows air outlining both the inside and outside walls of the bowel; b) falciform ligament sign is created by free air in a supine patient outlining the falciform ligament; c) the football sign which describes the shape of gas outlining the peritoneal cavity. On CT, small amounts of free air may be difficult to distinguish from intraluminal bowel gas, thus lung windows should be used to help differentiate.
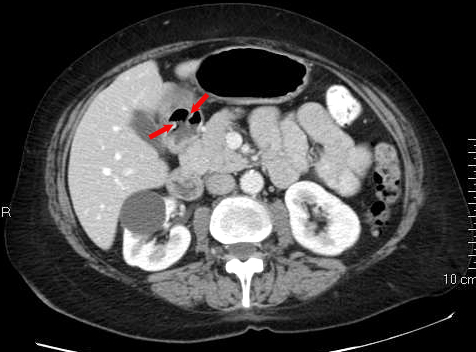
The above CT demonstrates free air in the peritoneum and shows the falciform ligament sign (arrows) and the double wall sign (arrowheads).
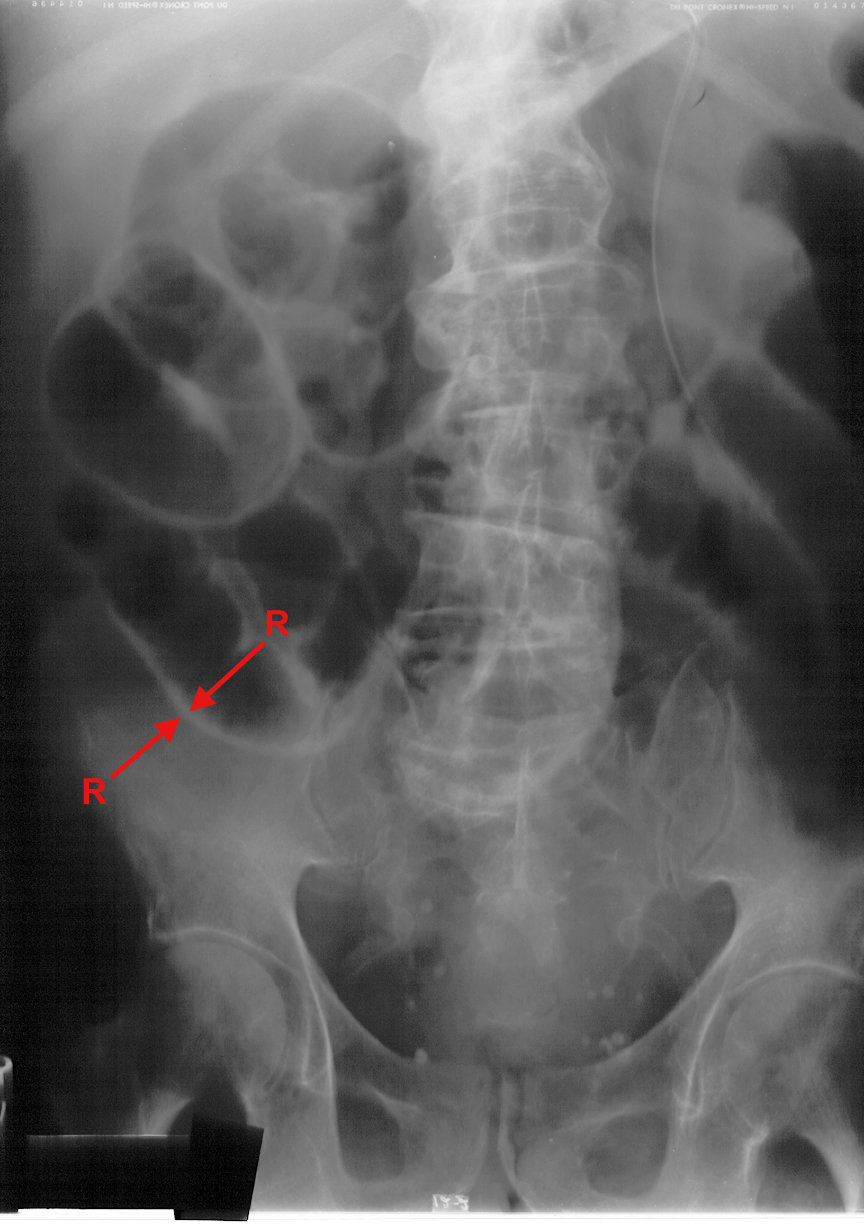
A) A) Supine abdominal film which demonstrates the double wall sign (Rigler's, outlined by arrows) due to free air in the peritoneum. B) Upright chest film demonstrates free air (A) under the domes of the diaphragm bilaterally.
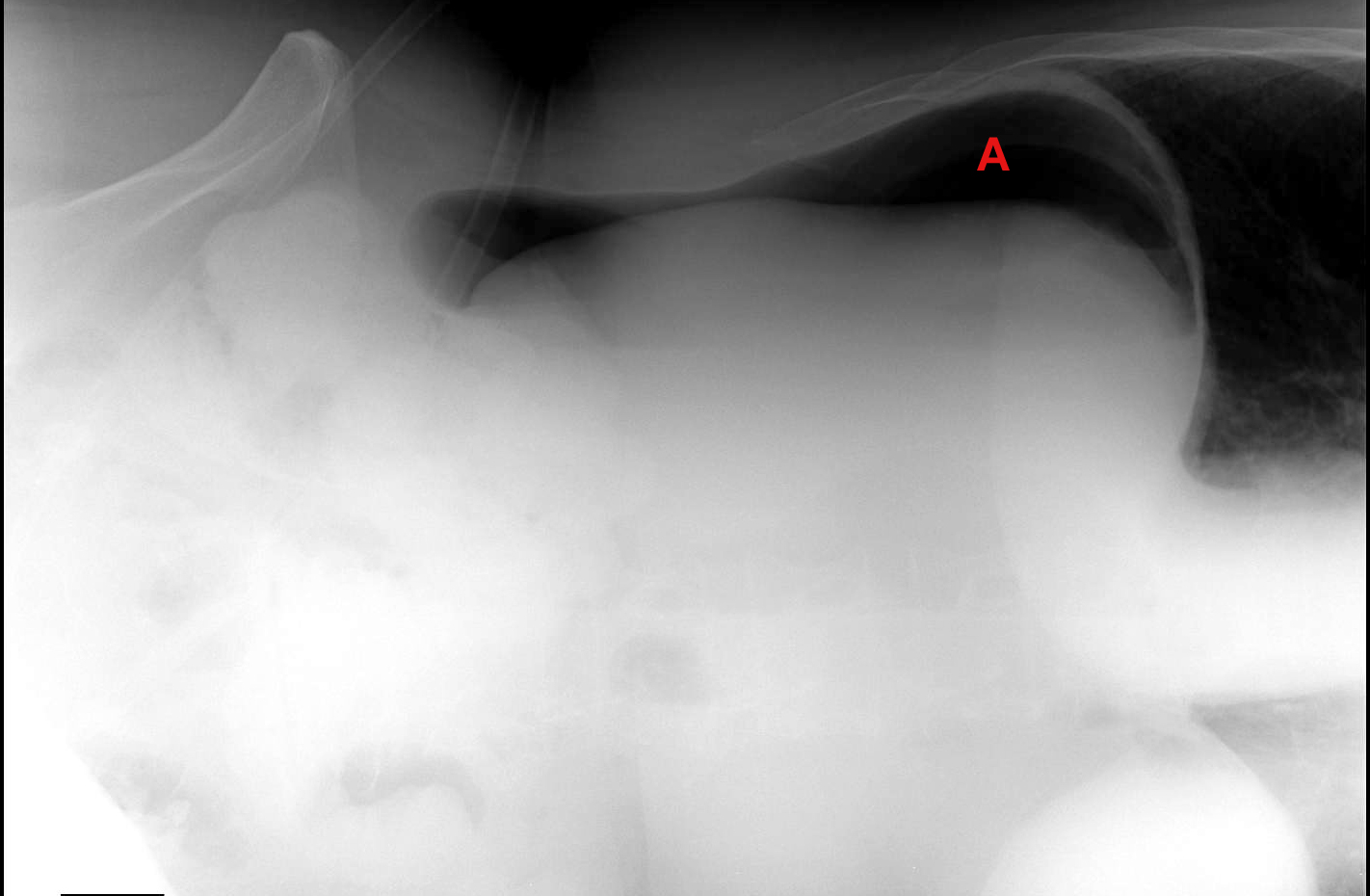
A) A) CT from a patient with a duodenal ulcer (arrows) B) Left lateral decubitus film from the same patient demonstrating pneumoperitoneum (A) resulting from perforation on duodenal ulcer after patient received steroids for treatment of COPD. |

 B)
B) 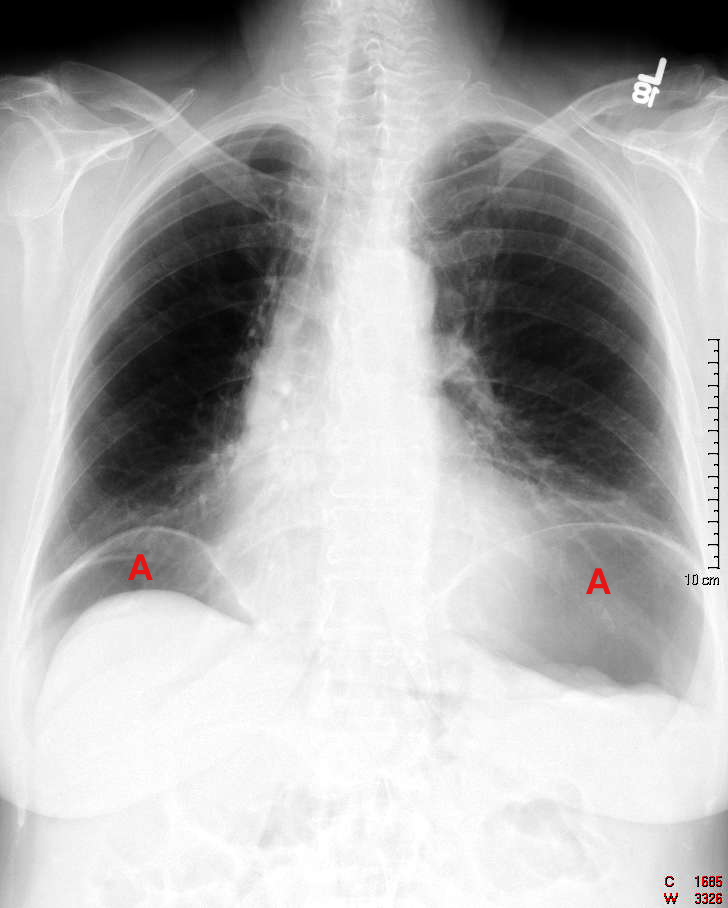
 B)
B)