GI Radiology > Peritoneum > Anatomy
Anatomy of Peritoneum
![]()
General |
|
The peritoneum is a serous mesothelial membrane similar to the pleura of the chest. It is made up of parietal peritoneum that lines the body wall and visceral peritoneum that lines the abdominal viscera. The abdominal organs are generally considered to be either intraperitoneal or retroperitoneal. The intraperitoneal organs are the stomach, spleen, liver, bulb of the duodenum, jejunum, ileum, transverse colon, and sigmoid colon. The retroperitoneal organs are the remainder of the duodenum, the cecum and ascending colon, the descending colon, the pancreas, and the kidneys. The mesothelium of the peritoneum normally acts as a barrier but it may also serve as a means of spreading disease including infectious and neoplastic processes.
As the peritoneum envelopes the abdominal organs, it folds over itself. These folds of peritoneum contain fat, lymphatics, and neurovascular supply to the abdominal viscera. The folds are classified as either ligaments, mesenteries or omenta. Ligaments are areas of peritoneum between two organs, i.e. the hepatoduodenal ligament, the splenorenal ligament etc.. Mesentaries are areas of bowel anchored to the posterior abdominal wall by peritoneum. There are two omenta, the greater and lesser omenta which are made up of the folds of peritoneum extending from the stomach's greater and lesser curvatures. The greater omentum is a typical site of spread of ovarian carcinoma.
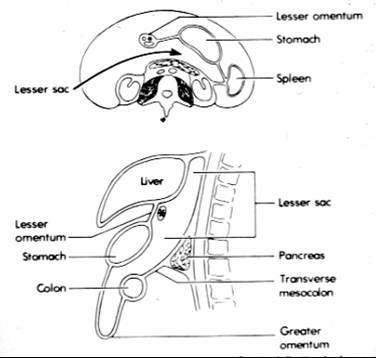
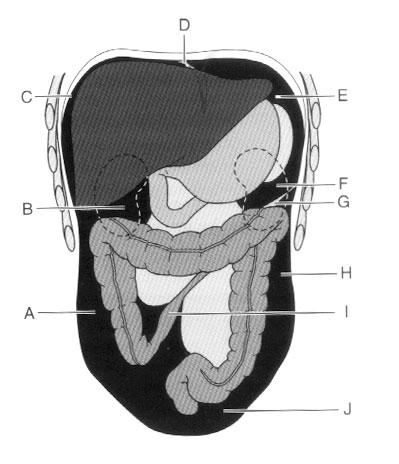
A. Right paracolic space (gutter), B. Hepatorenal recess (Morrison's pouch), C. Right subphrenic space, D. Falciform ligament, E. Left subphrenic space, F. Perisplenic space, G. Phrenicocolic ligament, H. Left paracolic space (gutter), I. Root of the mesentary, J. Cul de sac. The peritoneal cavity is a potential space divided into greater and lesser peritoneal cavities or sacs by the omenta. The lesser sac is isolated from the remainder of the peritoneal cavity and communicates with the greater sac only by the small epiploic foramne (Foramen of Winslow) on the right side. The boundaries of the lesser sac are: anteriorly the stomach and lesser omentum; posteriorly the pancreas; superiorly the liver and diaphragm; inferiorly the transverse colon, transverse mesocolon, and the greater omentum; on the left the spleen; on the right the epiploic foramen. This space is normally collapsed but can massively expand when filled with fluid (ascites, blood, pus).
A. Hepatorenal recess (Morrison's pouch), B. Right subphrenic space, C. Gastrohepatic ligament, D. Falciform ligament, E. Lesser sac, F. Gastrocolic ligament, G. Splenic flexure of the left colon, H. Phrenicocolic ligament, I. Anterior pararenal space, J. Spleen, K. Pancreas, L. Perisplenic space. In addition to the lesser sac, there are other areas within the peritoneal cavity that are clinically relevant. Ascites, blood, metastases, and abcesses are likely to collect in certain areas. The most dependent portion of the peritoneum in the upper abdomen in a supine position is the hepatorenal recess (Morrison's pouch). This area communicates freely with the right subphrenic space and and the pelvis via the right paracolic gutter. On the left side, the left subphrenic space communicates with the left subhepatic space but it is separated from the right subphrenic space by the falciform ligament and the left paracolic gutter by the phrenocolic ligament. In the upright position, the pelvis is the most dependent portion and free fluid, blood, infections, and metastases will often settle there. |