GI Radiology > Peritoneum > Fluid > Ascites
Ascites
![]()
|
Clinical Ascites is the accumulation of fluid in the peritoneal cavity. There are many different causes of ascites and in order to successfully treat ascites it is important to accurately diagnose the cause. The most common cause of ascites in the United States is liver disease, specifically cirrhosis. Other causes include fluid overload from CHF or renal failure, metastatic disease, peritonitis (malignant or infectious), ovarian neoplasms, trauma, surgery, or spontaneous hemorrhage. Ascites can often be diagnosed by careful physical examination, although those methods are not nearly as sensitive or specific as ultrasound. In order to accurately diagnose the nature and etiology of the ascites, paracentesis can be performed to evaluate the ascitic fluids appearance and content.
Radiological findings In order for ascites to be detected on plain film there must be more than 500 cc of fluid. It is important to remember that fluid can shift and move within in the peritoneum and will tend to accumulate in the most dependent areas. In the supine position fluid will accumulate in the hepatorenal recess (Morrison's pouch) which is between the anterior surface of the right kidney and the posterior surface of the right lobe of the liver. In the upright position it will accumulate in the pouch of Douglas which is posterior to the uterus in women and the bladder in men and anterior to the rectum. Findings of ascites on plain film include: a diffusely increased density of the abdomen or ground glass sign where the abdomen has a hazy appearance; indistinct margins of the liver, spleen, and psoas muscles due to fluid accumulation around these structures; medial displacement of the colon, liver, and spleen away from the flank stripe; bulging of the flanks; and "dog ears" which describes the appearance of fluid accumulating in the peritoneal recesses superolateral to the bladder.
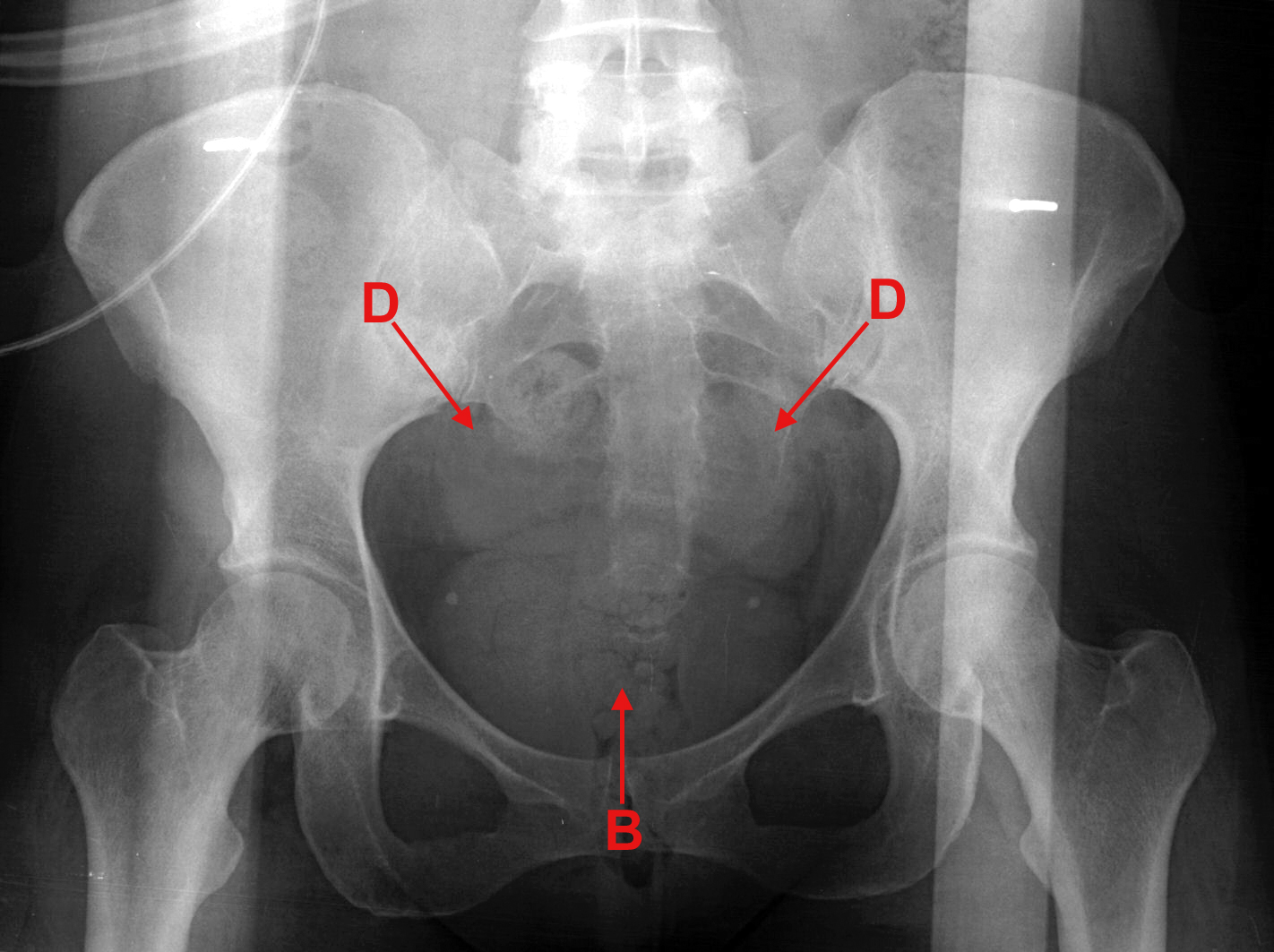
The above upright plain film demonstrates the finding of "dog ears" (D) above the bladder (B), due to accumulation of fluid in the recesses posterolateral to the bladder. Findings on CT include fluid densities in the recesses of the peritoneal cavity. The density of the fluid may help differentiate the nature of the ascites as serous fluid will be similar to water, exudative slightly more dense, and acute bleeding will be the most dense. It is important to remember that when evaluating fluid in the upper abdomen on CT that any fluid posterior to the diaphragm is pleural fluid and not ascites, whereas fluid within the diaphragm is ascites, however ascites cannot accumulate between the liver and the diaphragm as this is the bare area of the liver.
This CT demonstrates the relationship of the diaphragm, the peritoneum and the liver. (A) represents ascites in the peritoneal cavity, (B) is the bare area of the liver, (D) is the diaphragm, and (P) is pleural effusion.
CT showing ascites in the peritoneum. Note the peaking of fluid as it interfaces with the bowel. Ultrasound is the least expensive method for diagnosing ascites as it is very sensitive to detecting small amounts of fluid in the recesses. It may also help differentiate the nature of the ascites as simple ascites is anechoic whereas ascites with hemorrhagic, exudative, or neoplastic components may have floating debris.
Ultrasound image from a patient with cirrhosis shows nodular liver (L), and surrounding ascites (A). |