Gastrointestinal Radiology > Procedures > CT-Guided Perc. Gastrostomy > CT-Guided Perc. Gastrostomy (10)
CT-Guided Percutaneous Gastrostomy: A Tutorial
![]()
Procedure Variations
CT-guidance is only really necessary for the gastric access and gastropexy portions of the procedure. The fascial dilation and gastrostomy tube placement can be performed under fluoroscopic guidance once gastric access is achieved. Alternatively, the patient can be transferred to the endoscopy suite with the guidewire secured to the abdominal surface and looped in the stomach. If conversion to jejunostomy tube is anticipated, choose the gastric puncture site with this in mind. The gastrostomy tube should be placed in the gastric antrum or angled from the gastric body toward the antrum.
In patients with existing gastrostomy tubes that are suspected of of gastric contents or air leakage around the tube, approximation of the gastric abdominal wall can be performed. In this case, one would perform gastropexy adjacent to the existing tube.
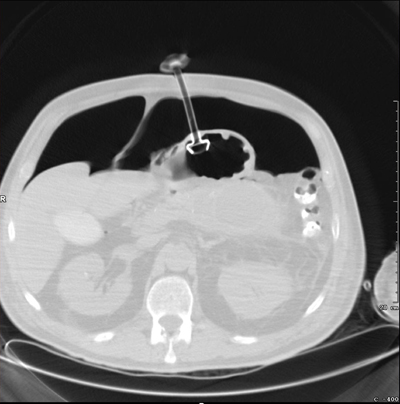
Image of gastrostomy tube with adjacent pneumoperitoneum
Post-Procedure Care
The patient should be observed until recovery from sedation is complete. The gastric anchor can be released immediately after the procedure or after two weeks. We prefer to leave the anchor in place for two weeks as the gastrostomy tract matures. To release the anchor, the suture is cut so that the anchor falls into the gastric lumen and passes through the gastrointestinal tract. Patients should be instructed on gastrostomy tube care. This care should be similar to other gastrostomy tubes, except that the relatively small lumen makes crushed pills less desirable than liquid medicine formulations.
Avoiding Complications
Potential complications of CT-guided gastrostomy include pneumoperitoneum, bleeding, colonic or liver puncture, peritonitis, and complications of sedation. Pneumoperitoneum is a relatively benign complication, and is expected when puncturing an air-filled, distended stomach. Excessive pneumoperitoneum is avoided by maintaining tension on the gastric anchor thread to keep the gastric and abdominal walls apposed. To prevent bleeding, one should be sure to avoid the epigastric vessels on the anterior abdominal wall. These are readily detectable on cross sectional imaging. Indeed, this is one of the advantages of CT-guidance. Additionally, distending the stomach with air lends some degree of protection from bleeding, as the gastric vessels occupy a smaller proportion of the stomach wall cross sectional area. Colon, lung, or liver puncture is avoidable by careful localization in planning and during the initial gastric puncture. Peritonitis can result from colonic puncture or excessive spillage of liquid gastric contents into the peritoneum. Keeping the stomach apposed to the abdominal wall and avoiding colonic puncture prevents this. Sedation complications are avoided by vigilant observance of the patient�s vital signs and responsiveness.
![]()
![]()