- After the catheter tip is in the antrum, turn
the patient into a steep left posterior oblique (LPO) position. Push the
catheter distally. When the tip of the torque cable is at the level of
the duodenal bulb, fix the position of the tip of the cable, and advance
the catheter off of it into the duodenal loop. Do not push the torque
cable into the duodenal loop, as perforation of the gut wall might
result.
(Drawings modified
from pamphlet, "Duodenal Intubation, A 5-Minute Method",
Cook, Inc.,
Bloomington, IN, copyright 1985)
- If, as sometimes happens, the catheter coils
in the fundus of the stomach, withdraw the catheter to the gastroesophageal
junction and again advance it as in steps 5 and 6. If this fails, remove
the torque cable and instill a small amount of barium or air through the
catheter to provide a visual marker of the gastroduodenal anatomy.
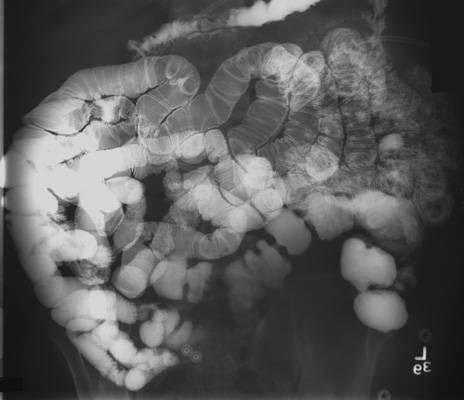
- After the catheter tip has been advanced into
the 4th part of the duodenal loop, return the patient to the supine
position. The final placement of tip of the catheter should be in the
region of the ligament of Treitz, either in the distal duodenal loop or
the proximal jejunum.
- Tape the catheter to the patient's nose to
prevent migration of the tube.
- If a balloon catheter is
used, the balloon may be inflated with as much as 15 ml of air to
prevent duodeno-gastric reflux. Of course, if the balloon is inflated,
it must be deflated prior to removal of the catheter at the end of the
procedure.
|