GI Radiology > Stomach > Pyloric Stenosis
Pyloric Stenosis
![]()
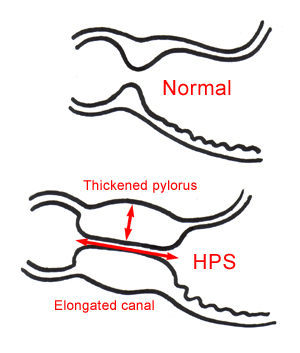
Hypertrophic Pyloric StenosisHypertrophic pyloric stenosis (HPS) results from idiopathic hypertrophy and hyperplasia of circular muscle fibers of the pylorus with proximal extension into the gastric antrum. It is technically an acquired rather than congenital condition. The US incidence is 3:1,000 live births. Males are more commonly affected than females by a ratio of 4:1. There is a bimodal distribution for age of presentation. Treatment is surgical by pyloromyotomy. | |
Infantile Form: Hypertrophy of the pyloric sphincter results in projectile nonbilious vomiting between the second and sixth weeks of life. Physical exam may reveal a palpable olive-shaped mass representing the hypertrophied pylorus. In the absence of this physical exam finding radiographic evaluation is indicated. Ultrasonography is the imaging modality of choice, followed by an UGIS if US findings are equivocal. |
 |
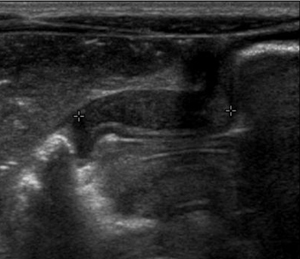
US Findings:
|
 |
UGIS Findings: (See Pediatric Imaging for examples.)
|
|