GI Radiology > Stomach > Neoplasms
Neoplasms
![]()
Gastric CarcinomaGastric carcinoma is the third most common GI malignancy after colorectal and pancreatic cancer, and represents the 6th leading cause of cancer deaths. The prevalence in the U.S. is approximately 24,000 cases per year. Predisposing factors for the development of gastric cancer include gastritis, adenomatous and villous polyp formation, gastrojejunostomy, partial gastrectomy, and pernicious anemia. Although they may present anywhere within the stomach, gastric carcinomas are most commonly located in the antrum or pylorus (50%); 60% are on the lesser curvature and 30% occur at the GE junction. Transpyloric spread to the duodenum rarely occurs (vs. 40% for lymphoma). Histologically, adenocarcinoma is most common making up 95% of gastric malignancies. Carcinoma Features:
| ||||||||||||||||||
|
||||||||||||||||||
The diagnosis is usually suggested by UGIS with confirmation by endoscopic biopsy. CT is useful in defining the extent of disease as hepatic or peritoneal metastases may be present. |
||||||||||||||||||
|
Radiographic Findings: UGIS
| ||||||||||||||||||
Radiographic Findings: CT
|
||||||||||||||||||
 |
 |
|||||||||||||||||
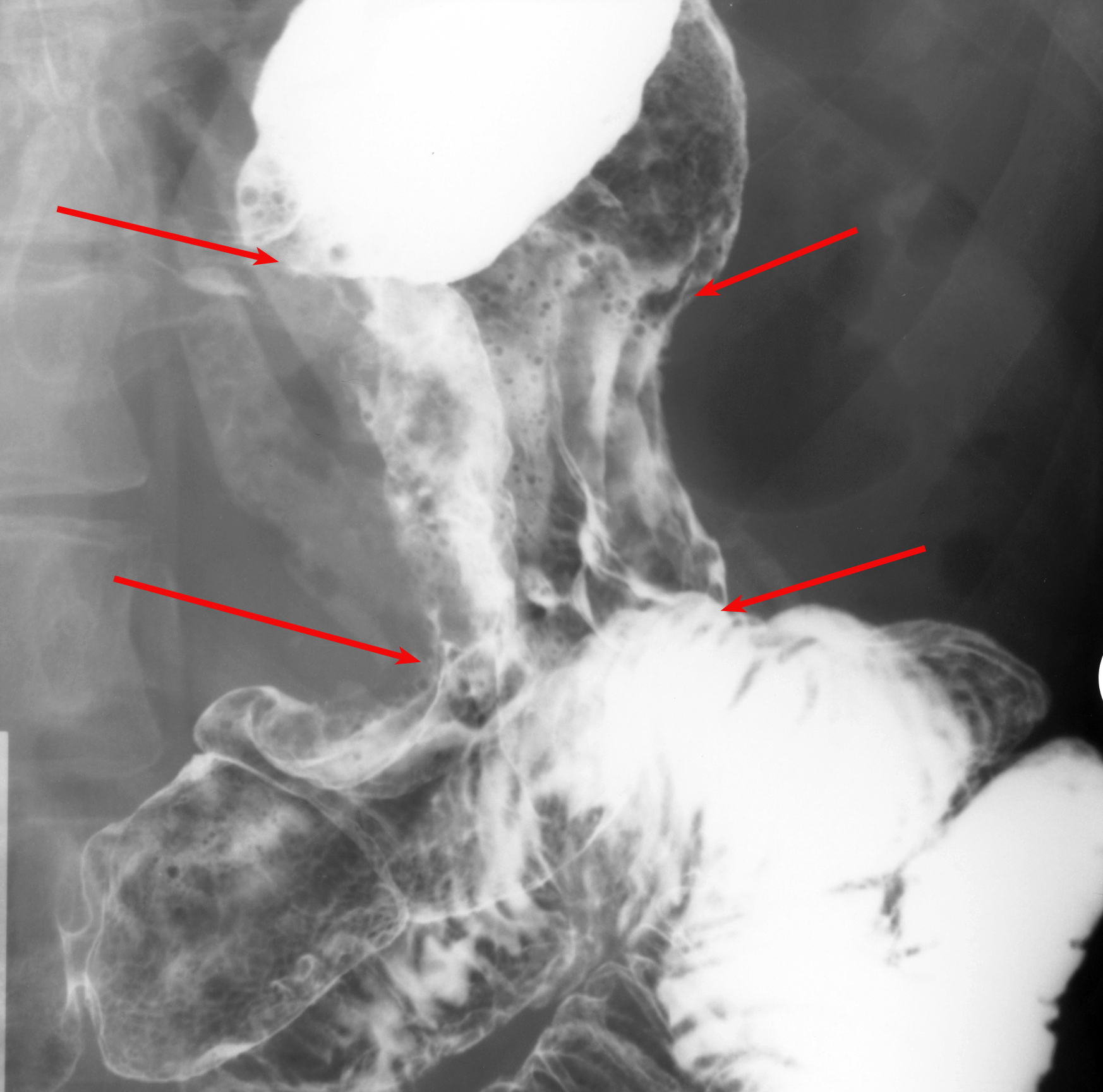
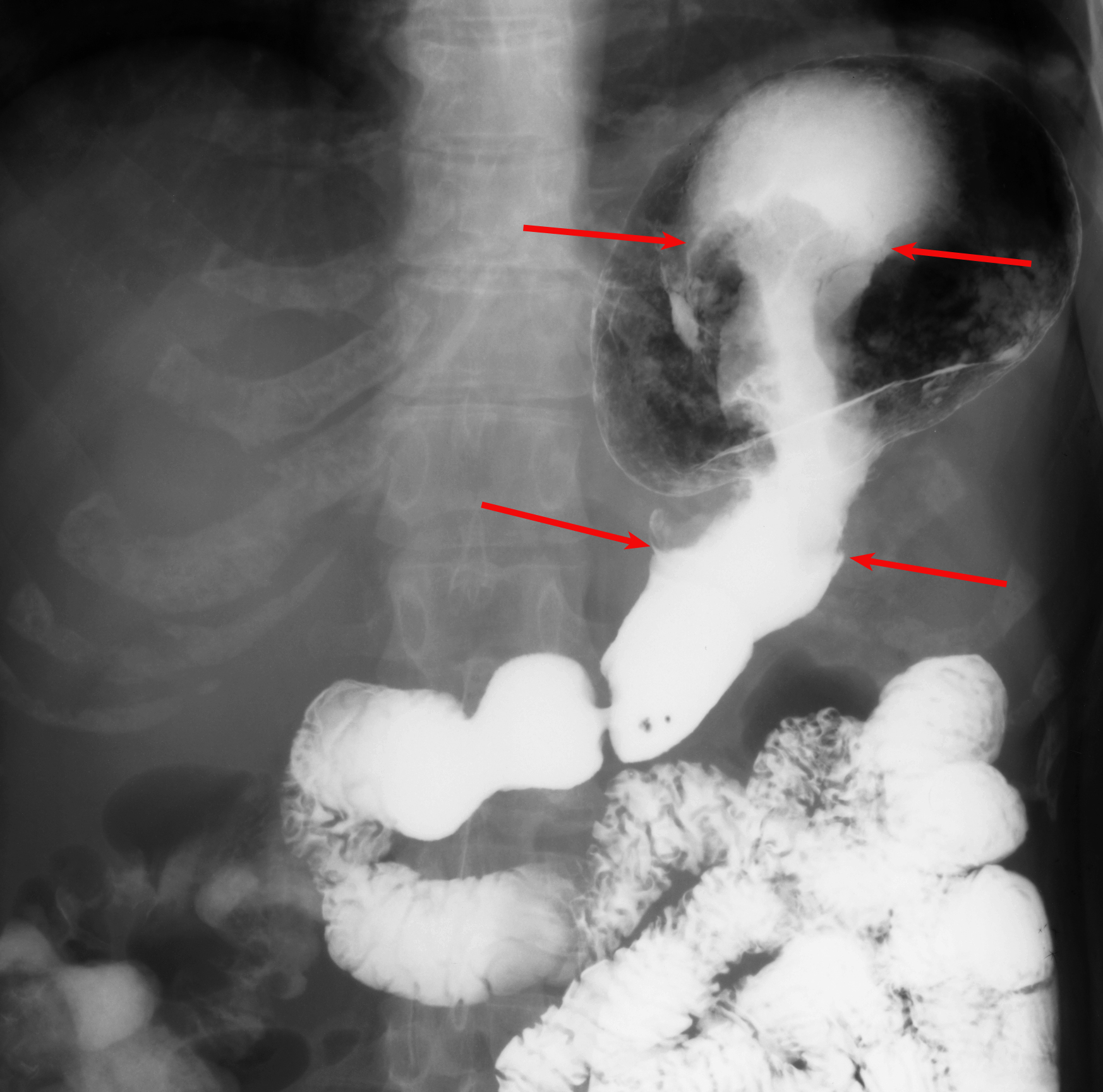
| A. UGIS double contrast study. The arrows outline the area of irregular mucosa which was caused by an invasive gastric carcinoma. | B. Single contrast study from the same patient showing the apple core appearance of the stomach due to the invasive gastric adenocarcinoma. | |||||||||||||||||