GI Radiology > Stomach > Neoplasms
Neoplasms
![]()
|
Gastrointestinal Stromal Tumors (GISTs) Gastrointestinal stromal tumors (GISTs) are submucosal spindle cell or epithelioid neoplasms. They share radiographic features common to many tumors, however are quite distinct histologically with all GISTs being positive for a tyrosine kinase growth factor receptor, C-kit (CD117). Proper diagnosis therefore requires tumor biopsy with immunohistochemistry. "GIST" is relatively new terminology; these tumors were previously called leiomyomas, leiomyoblastomas, and/or leiomyosarcomas. GISTs occur most often in the stomach (60-70%) and are preferentially located in the distal anatomic segments: body (39%), antrum (26%), pylorus (12%), fundus (12%), and cardia (10%). The majority of gastric GISTs are benign (80-90%); however, 10-30% are malignant, representing approximately 2% of all gastric malignancies. Although several factors increase the likelihood of malignancy in GIST, including an exogastric growth pattern, central necrosis, extension into adjacent organs, and metastases (most commonly liver and peritoneum; lymph nodes are rarely involved), differentiating between benign and malignant GISTs is unreliable based upon imaging studies alone, and is determined histologically according to the mitotic index�the number of mitotic figures per highfield microscopic examination. GISTs exhibit distinct growth patterns. Tumors may be endogastric (15%), exogastric (35%), or a combination of both (50%). Endogastric tumors tend to be submucosal or intramural; these are more likely to ulcerate while the tumor is small due to stretching of the overlying mucosa; bleeding typically leads to early diagnosis. Gastric outlet obstruction may occur if the tumor is located in proximity to the pylorus, again prompting early detection. Exogastric tumors are less likely to cause symptoms and are therefore larger at the time of diagnosis; a palpable mass is often appreciated upon physical exam. Definitive treatment of gastric GISTs is surgical resection. However, pharmacologic therapy with Gleevec, a tyrosine kinase inhibitor, has been indicated for the treatment of nonresectable or metastatic gastric GISTs. |
|
Radiographic Features: UGIS
|
Radiographic Features: CT
|
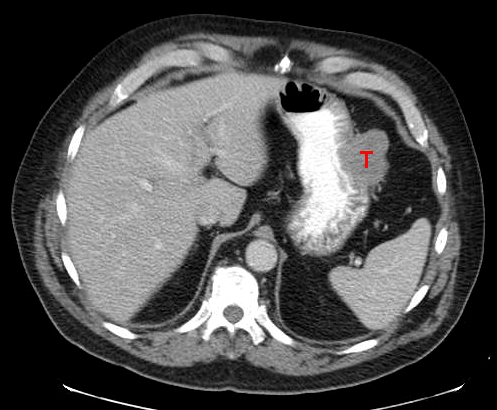
A CT image of a well-defined GIST confirmed by pathology. There is no apparent central necrosis and the tumor is not enhancing because only oral contrast was given. |