GI Radiology > Stomach > Other Conditions > Bezoars
Other Conditions
![]()
|
Gastric Bezoars Bezoars represent concretions of accumulated undigested material found in the stomach or other parts of the digestive tract. The ingested material is unable to exit the stomach because of large size, indigestibility, gastric outlet obstruction, and decreased gastric motility. Bezoars are composed mainly of vegetable matter (phyto), hair (tricho), or milk curds (lacto). Phytobezoars are the most common overall representing 55% of all bezoars. Trichobezoars are seen more frequently in pediatric patients and typically occur in young females with emotional problems. The overall incidence of gastric bezoars is low at approximately 0.4%. Predisposing conditions for bezoar formation include gastroparesis and prior gastric surgery. Clinical presentation varies but symptoms may include anorexia, abdominal pain, nausea, and vomiting. Diagnosis can be confirmed by UGIS , CT , or endoscopy. A worrisome complication is mucosal ischemia and necrosis caused by mechanical compression and obstruction. Management may include dissolution by oral ingestion of proteolytic enzymes, mechanical fragmentation via endoscopy, shock-wave lithotripsy (ESWL), or operative extraction. |
|
|
Radiographic Findings:
|
|
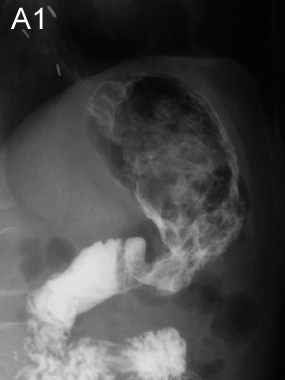
A1. UGIS demonstrating a 5cm filling defect in the gastric body. There is evidence of prior vagotomy, as indicated by surgical clips (arrowheads), which would contribute to delayed gastric emptying. Show labels. |
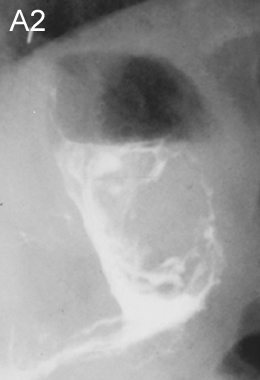
A2. Spot film shows contrast outlining the defect, suggesting it is not attached to the gastric wall. Upper endoscopy confirmed the diagnosis of a phytobezoar. |
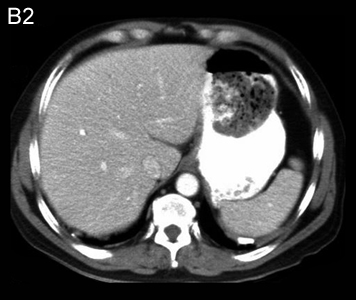
B1. Upright abdominal plainfilm obtained for evaluation of chronic nausea and vomiting. A large opacification within the gastric body was noted. |
B2. Single axial CT image from the same patient demonstrates a heterogeneous mass floating within the lumen of the gastric body consistent with a bezoar. Note that contrast surrounds the concretion. The patient's symptoms were produced by intermittent gastric outlet obstruction caused by a large phytobezoar. |