GI Radiology > Stomach > Psuedotumors
Pseudotumors
![]()
|
Gastric Varices Gastric varices are collateral veins that dilate in response to impeded venous flow. They are usually seen in association with esophageal varices and portal hypertension secondary to cirrhosis. Isolated gastric varices are typically due to splenic vein thrombosis (i.e. from pancreatic cancer or pancreatitis). When portal hypertension develops, the alternate sites of gastric venous collateral circulation include the mesentery, the retroperitoneum, the small and large bowel, and the regions adjacent to the diaphragm and gallbladder. The most common collateral channel demonstrated is through the coronary or left gastric vein which anastomoses with the esophageal and paraesophageal veins (porto-systemic circulation). Commonly accompanying this are abnormally dilated short gastric veins which pass from the splenic vein to encircle the gastric fundus and form gastric fundal varices. UGIS has a 70-90% detection rate. | |
|
Radiographic Findings:
|
|
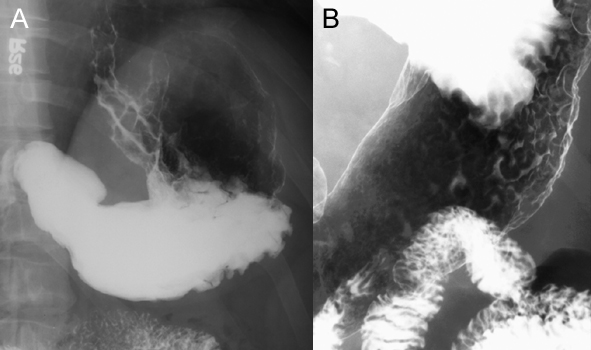
A. UGIS demonstrating marked lobulated filling defects (arrow-heads) in the esophagus, cardia, fundus, and along the greater curvature of the stomach (arrows). Show labels. B. UGIS visualizing marginal longitudinal serpiginous filling defects (arrow-heads) and a single engorged vein en face (circle). Show labels. |
 |
| CT with IV and oral contrast. Single axial image of the abdomen demonstrates retrogastric varices, representing a portion of the fundal venous plexus and short gastric veins. |  |