Pediatric Radiology > Musculoskeletal > Trauma > Anatomical Locations of Common Fractures
Anatomical Locations of Common Fractures
![]()
| The
most commonly encountered locations for pediatric fractures include the
wrist and elbow. With regards to the wrist, the most common scenario involves
a buckle or transverse fracture of the distal radial metaphysis with or
without involvement of the distal ulnar metaphysis. Note that roughly
25-30% of all physeal fractures occur in the wrist. The pronator
fat pad (seen on a lateral view of the forearm as a thin line of fat with
a mild convex border) is often displaced or obliterated if a fracture is
present.
|
|||||||||
|
Injuries involving the elbow are often secondary to hyperextension sustained from falling on an outstretched hand. In adults, this mechanism of injury would result in a fracture of the radial neck, whereas supracondylar fractures are more prevalent in the pediatric population. Radiographs of supracondylar fractures demonstrate posterior displacement of the distal fragment such that the anterior humeral line does not bisect the middle third of the capitellum (see figure below). Fracture lines are often seen through the anterior cortices on lateral views. Joint effusions are also typically present as evidenced by displacement of the posterior fat pad. Normally, this fat pad lies within the olecranon fossa and is not seen on the lateral view. A joint effusion may also elevate the anterior fat pad. This fat pad is often normally visualized, but with an effusion, it may become more prominent. 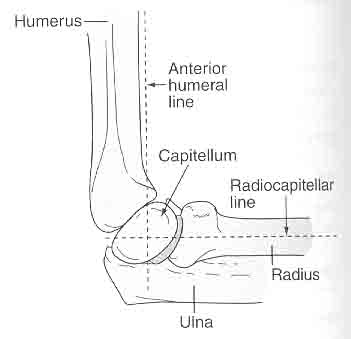
Other prevalent elbow injuries include fractures of the lateral epicondyle and avulsion injuries of the medial epicondyle ("little league elbow"). With avulsion injuries, which comprise roughly 10% of all elbow injuries, there may be some displacement. It is necessary to know the sequence of ossification of the elbow to avoid mistaking a displaced apophysis for one of the ossicles of the elbow. The predictable order of elbow ossification is:
|







| Toddler's fractures are non-displaced oblique or spiral fractures of the midshaft of the tibia. They are found in children who have just recently begun to walk. Most children present refusing to bear weight or walk on the involved extremity. These fractures are often best viewed on oblique images. |
 |
Toddler's Fracture in a young patient who recently became ambulatory. AP radiograph shows a non-displaced spiral fracture of the tibial shaft. |
![]()
![]()