CT Pulmonary Angiography > Pitfalls
Pitfalls of CTPA
![]()
Anatomic Pitfalls: PA�s run with bronchi, PV�s run independent, Unopacified veins, Mucoid impaction, Lymphadenopathy and perivascular tissue, Other pathologies (Shunts, Sarcomas)
Imaging Artifacts: Streak artifacts, Motion artifacts, Improper bolus timing, inconsistent (�fractured�) bolus Edge-enhancing reconstruction algorithm, Inadequate window settings, Patient size
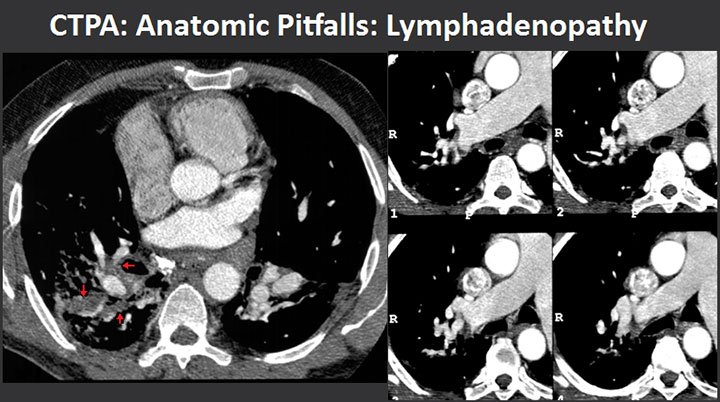
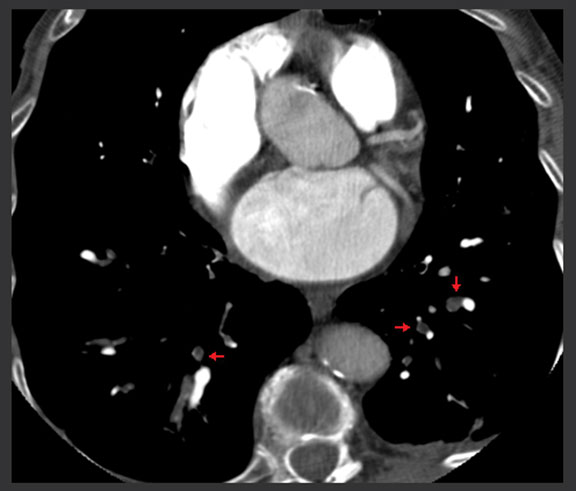
Computed tomography pulmonary arteriography: pitfalls - lymphadenopathy. Lymphadenopathy in a patient with silicosis and shortness of breath mimicking acute pulmonary embolus. There are multiple lymph nodes adjacent to vessels that occasionally could impose problems differentiating from partially organized thrombus (arrows).
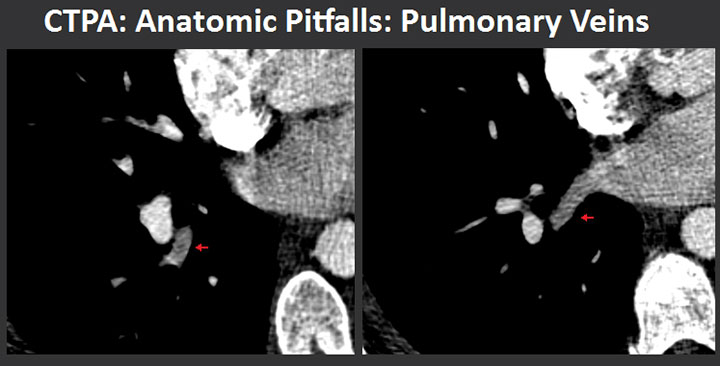
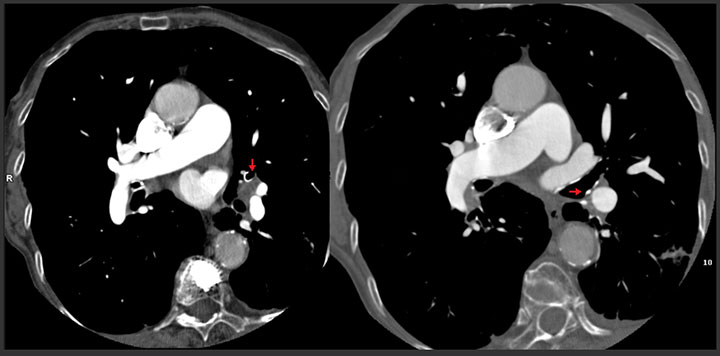
Computed tomography pulmonary arteriography: pitfalls - nonopacified pulmonary vein. Image on the left has been occasionally misdiagnosed as acute pulmonary embolus (arrow). However, following the brnach towards the left atrium helps clarify this question in all cases (arrow).
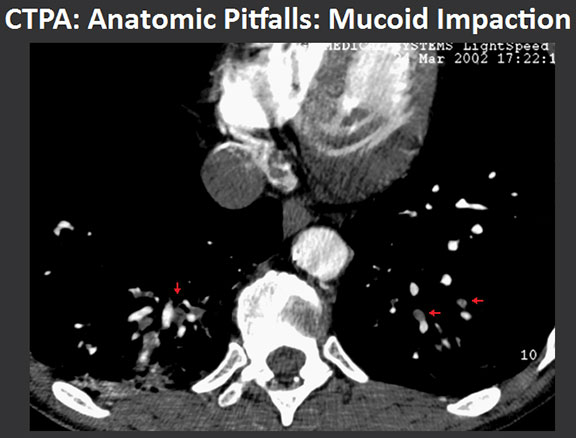
Computed tomography pulmonary arteriography: pitfalls - mucoid impaction. This shows the typical appearance of mucous-filled bronchi (arrows) adjacent to the enhanced arteries. This finding should not be mistaken for pulmonary embolism.
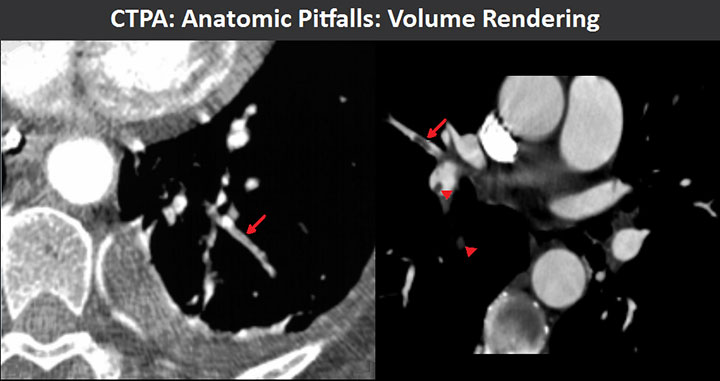
Computed tomography pulmonary arteriography: pitfalls - volume rendering. (Left) Pulmonary arteries that run in-plane parallel with bronchi can occasionally appear less dense than the arteries running perpendicular to the imaging plane. This is caused by partial volume averaging of the air-filled bronchi into the pulmonary artery, thus artificially reducing its density (arrow). Reconstruction of the dataset with thinner slices and/or oblique perpendicular multiplanar reconstructed images usually help resolve this issue. (Right) True pulmonary embolus in a small branch to the middle lobe running in-plane (arrow). There are also other emboli (arrowheads).
![]()
![]()