CT Pulmonary Angiography > Pulmonary Embolus > Technique
Technique used for CTPA
![]()
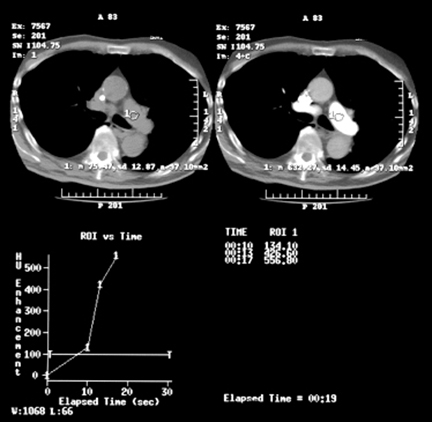
For CTPA at our institution, we use a multidetector CT scanner. We use a collimation of 1.25 mm with a beam pitch of 1.35 (slice pitch 10.8; US Mode) and 0.5 sec. gantry rotation time. This results in an acquisition time of 6.4 seconds for 160 mm z-axis coverage, which is sufficient in most patients to cover the lungs from the base to the apex. The data is initially reconstructed without overlap, in cases with questionable or subtle findings suspicious for subsegmental PE, we reconstruct the raw data with 0.6 mm interval resulting in approximately 50% overlap. In general, optimal results are achieved on multislice CT scanners using the thinnest collimation available. For bolus timing an automated bolus detection system (SmartPrep) is used routinely. We inject 100 ml of nonionic contrast (density 320-350 mg I/ml) at 4 ml/sec using a power injector. Once the Hounsfield units (HU) in a predefined region of interest in a dynamic scan through the main pulmonary arteries exceed a preset threshold (100 HU), the CTPA acquisition is started. Scanning is performed in caudocranial direction during a breath hold. The axial images are reviewed on a workstation, where interactive features like image scrolling and window setting adjustments on the fly improve the ability to interpret the data. In addition, the large number of images generated (140-280 per study) makes review from hardcopies impractical and prohibitively expensive. Image reconstruction algorithms like Multiplanar Reformatting (MPR) are also used on a workstation.
![]()
![]()