Emergency Ultrasound > Testicular Pain > Epididymitis
Testicular Pain - Epididymitis
![]()
Clinical
Epidydimitis is usually caused by Chlamydia ssp., but Neisseria gonorrhoeae is also a common pathogen. It is most often found in post-pubertal, sexually active males. It presents as a tender and erythematous (acutely inflamed) epididymis. Urethral discharge, dysuria, fever and pyuria may also be present.
Exam
Begin with the patient in the supine position. Place a white towel below the testicle. Use a second towel to cover the underside of the penis and move it to the lower abdomen so the testicles are easily accessible.
Always use a 7.5 MHz linear transducer to look at flow in the testicle.Color settings: put on small parts of testicle.The filter must be on 1 or 2 and the color velocity scale on the lowest possible setting for maximum sensitivity.It is absolutely essential to compare to the opposite presumed normal testicle to visualize its vessels so that you know your color settings are right and you are not just getting color noise.
Gray Scale
Obtain long and transverse scans through the scrotum. Include upper, mid, and lower testicle in transverse. Measure the testicles and the epididymis (abnormal is > 1cm). Show hydrocele if present.
Color Doppler
Document color flow to the testicles. Note any increased flow to the epididymis or testicle, which may mean epididymitis or orchitis respectively.
Sonographic Findings:
1) Epididymis is swollen and decreased in echogenicity.
A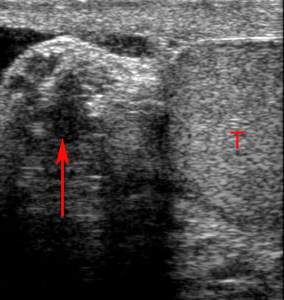 B
B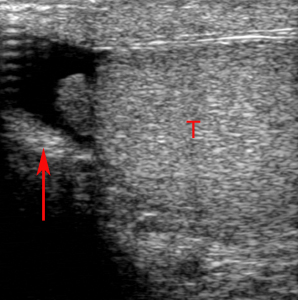
The painful right (A) epididymis (red arrow) is enlarged and hypoechoic compared to the asymptomatic left (B) epididymis (red arrow). Each testicle is indicated by T.
2) Doppler demonstrates asymmetric hypervascularity of the affected epididymis reflecting arterial and venous dilatation.
A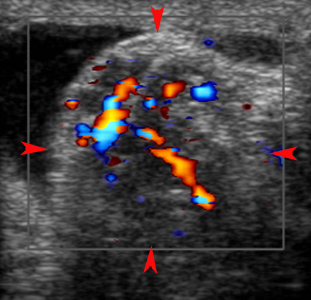 B
B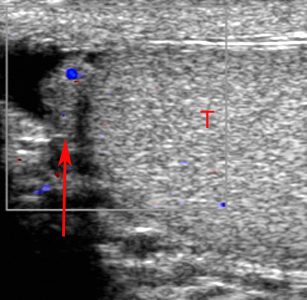
Acute Epididymitis. Color Doppler images show marked increase in vascularity in the right (A) epididymis (red arrowheads) compared to the left (B) epididymis (red arrow). T indicates left testis.
![]()
![]()