GI Radiology > Appendix > Imaging Modalities
Imaging Modalities
![]()
Introduction |
|
The majority of appendix pathology (appendicitis) is diagnosed clinically, based on a combination of clinical history and physical findings. Imaging becomes important in the cases that present with atypical or equivocal clinical findings. Several modalities may be involved in the diagnosis of appendicitis, including conventional abdominal radiographs, ultrasound and/or CT. |
Plain Films |
|
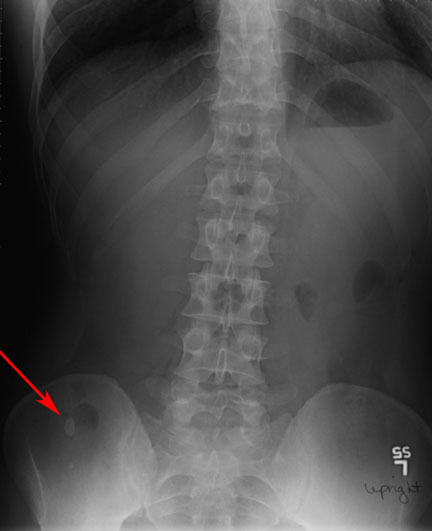
Plain films are often used as a screening tool for patients presenting with complaints of abdominal pain. Although, they are highly non-specific for appendicitis, one can often see evidence of inflammation. This includes indistinctness of the right psoas muscle margin, scoliosis with splinting of the spine to the right side, focal obliteration of the properitoneal fat line. 10-15% of the time a calcified appendicolith can be seen, which in a symptomatic child has a high correlation with acute appendicitis. Very rarely, free air in the peritoneal cavity will be seen secondary to rupture of the appendix, which is an indication for immediate surgical treatment.
Anteroposterior abdominal radiograph shows a calcified appendicolith in the right lower quadrant (arrowhead). The bowel gas pattern is nonspecific, note the loss of the psoas margins bilaterally, this is a marker of inflammation.
|
Computed Tomography |
|
Normal appendix can usually be identified on CT. Unfortunately the position of the appendix is highly variable, which can often make it difficult to identify for a novice radiologist. The appendiceal wall, if visible, should be <2mm thick. Surrounding fat should be homogenous without stranding. The abnormal appendix is distended, thick walled, and >6 mm diameter. Stranding of the periappendiceal fat is often present and is an indicator of inflammation. Enhancement of appendix wall with contrast indicates hyperemia. Adjacent fluid may represent inflammation, rupture, or abscess. Cecal wall thickening with oral contrast trapped between the two walls is known as the "arrowhead" sign, and is a marker of inflammation.
Abdominal CT scan demonstrating a fluid filled appendix. Note the enhancement of the appendiceal wall as well as free fluid surrounding the appendix.
|
Ultrasound |
|
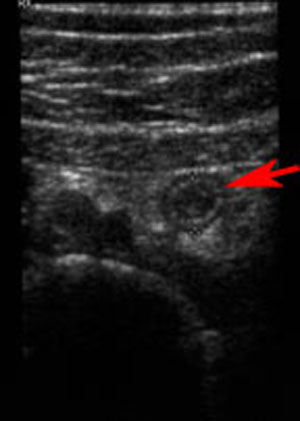
Ultrasound is the best test for pediatric patients, young, and pregnant females. No ionizing radiation or contrast needed, thus there is less risk for the patient. The normal appendix is usually not seen on ultrasound. The abnormal appendix is seen as a blind ending tubular structure arising from cecal base and is non compressible with pressure from the transducer. A cross section diameter greater then 6 mm is abnormal.
Abdominal ultrasound showing the appendiceal lumen (arrowhead) surrounded by free fluid, suggestive of inflammation. Remember the normal appendix should NOT be visualized on ultrasound.
|
Ultrasound vs CT |
|
There are differing opinions as to which test should be done first. Advantages of CT include superior sensitivity and accuracy and ability to demonstrate alternative diagnoses. Several studies demonstrate reduced negative laporotomy rates when CT is used. Disadvantages include use of IV contrast, exposure to ionizing radiation, GI discomfort (oral contrast) and delay waiting for results. In certain population, children and in young or pregnant females, ultrasound is preferred over CT due to low cost, quick availability and lack of exposure to ionizing radiation and IV contrast. If ultrasound is negative or equivocal, proceed to CT. Most would recommend going to CT directly for all other patients. |