GI Radiology > Appendix > Neoplastic
Neoplastic Diseases of the Appendix
![]()
Introduction |
|
Primary appendiceal neoplasms are very uncommon, found in 0.5-1.0% of appendectomy specimens. Most are seen in middle aged adults (with the exception of carcinoid tumors), and 30-50% will manifest with signs of acute appendicitis which lead to abdominal imaging. Other manifestations include asymptomatic mass, GI bleeding, or increasing abdominal girth. |
Carcinoid Tumor |
|
Carcinoid tumors are derived from sub-epithelial neuroendocrine cells, and may represent up to 80% of all appendiceal neoplasms. They are most often discovered incidentally at surgery or pathology and tend to occur in younger patients when compared to other appendiceal neoplasms. In the setting of acute appendicitis, co-existing carcinoid tumor are obstructing in only 25% cases, this is chiefly due to the fact that 70% of tumors are found in distal third of appendix and are less then 1 cm in size. Although, all carcinoid tumors are potentially malignant, metastatic disease from carcinoid with appendiceal primary site is exceedingly rare. Increase risk of malignancy exists if the tumor is greater then 2.0 cm. Carcinoid tumors will usually manifest as acute appendicitis, however on CT or US the tumor itself may not be appreciated due to its small size. Clues include calcification(mimicking appendicolith) or a diffuse infiltrative pattern, if the tumor is large enough. |
Mucinous Epithelial Neoplasms |
|
Although mucinous neoplasms are less common then appendiceal carcinoid tumors, they are more likely to be detected at imaging, due to their larger size and corresponding higher rate of complications. The majority of epithelial tumors of the appendix are mucin rich, demonstrate circumferential mucosal involvement, and have a strong propensity to form mucoceles. Regardless of whether they are benign or malignant, the majority of mucinous neoplasms that are resected have formed mucoceles. It is quite difficult, if not impossible to, differentiate a benign vs. malignant mucocele based on imaging. Clinical manifestations are similar to carcinoid tumors, but malignant tumors may also invade adjacent organs or cause increasing abdominal girth from extension into the peritoneal cavity (pseudomyxoma peritonei). CT is imaging modality of choice, with the diagnosis depending primarily on detection of the resulting mucocele. Curvilinear mural calcifications in a hypodense mass are highly suggestive of a mucocele. Intraluminal gas bubbles or air-fluid level within the mucocele are diagnostic for superinfection. Pseudomyxoma Peritonei can be caused by mucocele rupture or transmural extension. Typical imaging features include widespread, heterogeneous peritoneal locules that displace hollow viscera or produce scalloping effect on solid organs. Be aware the ovarian tumors are also a known cause of pseudomyxoma peritonei.
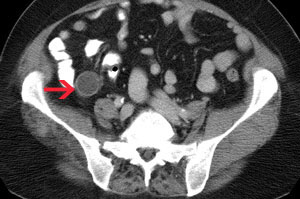
Abdominal CT showing a cystic lesion in the expected region of the appendix. A second image from the same patient shows mural calcifications within the lesion. This is highly suggestive of a mucocele from a mucinous adenocarcinoma(although pathology on this patient revealed this lesion to actually be a mucinous cystadenoma).
Abdominal CT demonstrates scalloping of the liver due to pseudomyxoma peritonei. Additionally a focal area of peritoneal carcinomatosis(red arrowhead) can also be appreciated.
|
Colonic type (non mucinous) Epithelial Neoplasms |
|
These tumors are quite rare. They comprise only 2% of adenomas and 7% of adenocarcinomas of appendix. They tend not to form mucoceles and generally manifest clinically with appendicitis related to malignant tumor obstruction. At CT, a soft tissue mass involving the appendix, but demonstrating no mucocele formation is seen. |