GI Radiology > Appendix > Inflammatory
Appendicitis
![]()
Introduction |
|
Approximately 20% of patient visits to the emergency department for non-traumatic acute abdominal symptoms are related to the appendix. In fact, appendicitis is the most common reason for emergency abdominal surgery in the young adults and especially in the pediatric population. Therefore it is important to be able to quickly and correctly identify pathology of the appendix and treat it. |
Pathophysiology |
Appendiceal obstruction leads to venous and lymphatic obstruction producing an edematous, inflamed appendix. The resulting ischemia and mucosal breakdown allows bacteria to invade the appendix wall. Gangrene with rupture and peritonitis may ensue. |
Clinical Presentation |
|
Laboratory Data |
|
Diagnosis |
Most often diagnosed clinically, imaging can help in atypical of equivocal cases
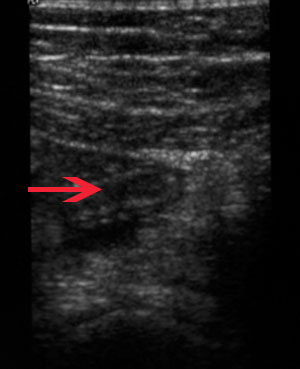
Abdominal ultrasound showing an elongated, blind ended tube. Highly suspicious for appendicitis.
Abdominal CT demonstrating a fluid filled appendix, surrounded by an appendiceal abscess(fluid around the appendix surrounded by an enhancing rim.)
|
Differential Diagnosis for RLQ pain |
|
Treatment |
For uncomplicated cases proceed directly to appendectomy. If there is an abscess present, drain the abscess percutaneoulsy and perform an interval appendectomy in 4-6 weeks. |