GI Radiology > Esophagus > Neoplasms
Neoplasms
![]()
Leiomyoma |
|
Clinical Leiomyomas make up approximately 50% of all benign esophageal tumors. About 60% of the lesions are located in the distal third of the esophagus, 30% in the middle third, and 10% in the proximal third. The tumors consist of intersecting bands of smooth muscle and fibrous tissue in a capsule. They appear as discrete submucosal masses ranging from 2 to 8 cm in size. Most patients with esophageal leiomyomas are asymptomatic. However, it patients do become symptomatic they often complain of intermittent, worsening dysphagia, substernal pain, vomiting, or weight loss. Leiomyomas are slowly progressive, therefore it may be years before a patient notices any symptoms. Treatment of choice for esophageal leiomyomas consists of surgical enucleation.
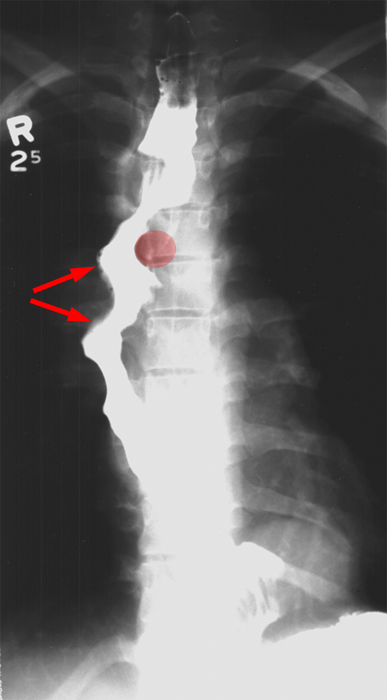
Radiological findings On chest films, leiomyomas may be recognized as a soft tissue mass in the posterior mediastinum or by punctuate areas of calcification in the tumor. A calcified esophageal mass is pathognomonic of a leiomyoma. In contrast studies, the leiomyomas appear as discrete submucosal masses with round or ovoid filling defects sharply outlined by barium. When viewed in the lateral projection, the lesions have a smooth surface with their upper and lower borders forming abrupt right or obtuse angles with the adjacent esophageal wall. Larger leiomyomas may occasionally cause some compression of the lumen significantly enough to narrow the lumen. Occasionally, the leiomyomas near the GE junction, may also involve the gastric cardia and fundus. These lesions tend to cause severe dysphagia because of its distal obstruction.
In
this image, the ovoid filling defects caused by the leiomyoma. The smooth
surface and obstuse angles formed are characteristic of submucosal masses.
|