GI Radiology > Esophagus > Neoplasms
Neoplasms
![]()
Squamous Cell Carcinoma |
|
Clinical Espophageal carcinoma constitutes only about 7% of all GI carcinomas. The 5-year survival rate for esophageal carcinoma is less than 10%. A majority of esophageal cancers are of the squamous cell type. Tobacco use and alcohol consumption are two of major risk factors contributing to esophageal cancer. There are also some esophageal conditions that are thought to predispose patients to the development of squamous cell esophageal cancer: achalasia, lye strictures, head and neck tumors, celiac disease, Plummer-Vinson syndrome, radiation therapy, and tylosis (rare autosomal dominant disease characterized by hyperkeratosis of the palms and soles. Squamous cell cancers are evenly distributed between upper, middle, and lower thirds of the esophagus. Metastases is possible either by direct extension, lymphatic or hematogenous spreading. Patients only complain of dysphagia after the lumen has lost 50 to 75% of it's circumference, and by that time it is likely that the malignancy has spread to surrounding structures. Other common findings include odynophagia, anorexia, weight loss, and persistent substernal chest pain unrelated to swallowing.
Radiological findings Early: Double contrast esophagography is the study of choice. At the early stages, esophageal cancers appear as small, protruding lesions less than 3.5 cm in diameter. They can be small plaque-like lesions with central ulceration or small, sessile polyps with a smooth contour. They may also be visualized as superficial, depressed lesions that cause irregularity, nodularity or ulceration of the esophageal mucosa.
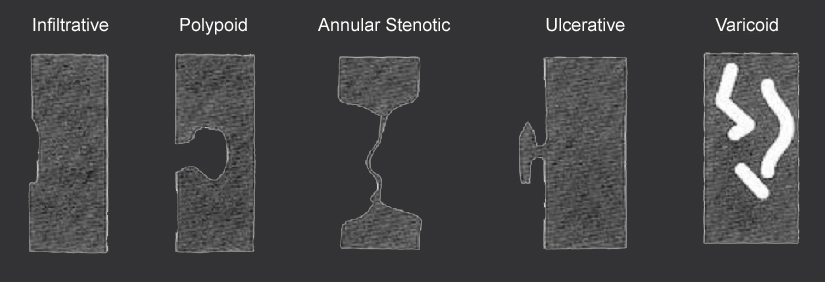
The above image is a graphical represenation depicting the different patterns of esophageal squamous cell cancer.
Late: On plain films, one might observe a widened mediastinum, hilar or retrocardiac mass, tracheal deviation, widened retrotracheal stripe (> 3mm), and an air-fluid level in the esophagus. On contrast studies, esophageal cancer may appear as an infiltrating, polypoid, ulcerative, or varicoid lesion. Infiltrating cancers show irregular narrowing of the lumen with an associated nodular or ulcerated mucosa with well-defined borders. Polypoid lesions are usually greater than 3.5 cm in diameter and appear as lobulated or fungating intraluminal masses with possible areas of ulceration. Ulcerative carcinomas appear as well-defined meniscoid ulcers with a radiolucent rim of tumor surrounding the ulcer. Varicoid carcinomas mimic esophageal varices and therefore appear as thickened, tortuous, or serpiginous filling defects because of the submucosal spread of the cancer.
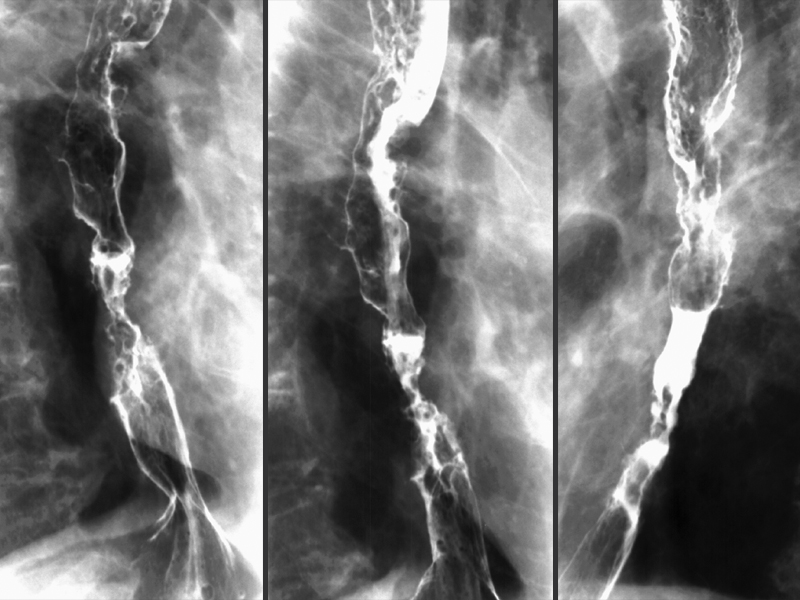
In the esophagram in image "A" we can see a Schatzki ring (red arrows) and filling defects (yellow arrows) proximal to the ring which was found to be squamous cell cancer. Images "B" and "C" show the same findings in a close-up view.
In these images, we can see an irregular stricture in the esophagus with ucleration of the esophageal mucosa. Also noticed the shouldered margins of the lesions.
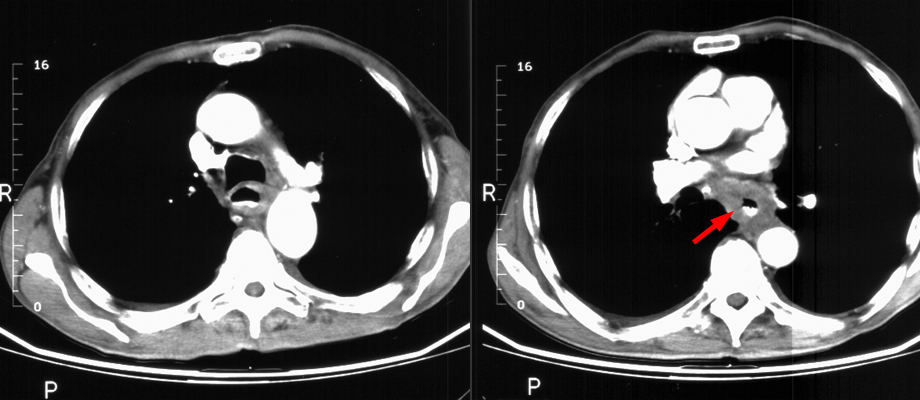
In the above CT images, one can see circumferential thickening of the esophageal wall (annular lesion). |