GI Radiology > Esophagus > Structural Abnormalities
Structural Abnormalities of the Esophagus
![]()
Foreign Bodies/Food Impaction |
|
Clinical 80% of pharyngeal or esophageal foreign body impactions occur in children, who accidently ingest coins, toys, etc. In adults however, animal/fish bones or large boluses of meat cause most foreign body impactions. Bones tend to become impacted in the pharynx near the cricopharyngeus muscle, where as meat boluses usually in the distal esophagus above the gastroesophageal junction. 80 to 90% of these foreign bodies pass spontaneously, but the others may require some sort of intervention. In pharyngeal impactions, patients may complain of dysphagia or a sensation of a foreign body being "stuck in [their] throat." In meat bolus impactions, patients may complain of sudden onset of chest pain, odynophagia, or dysphagia. The risk of esophageal perforation in foreign body impaction is less than 1%, however, the risk increases significantly if the foreign body remains lodged for greater than 24 hours.
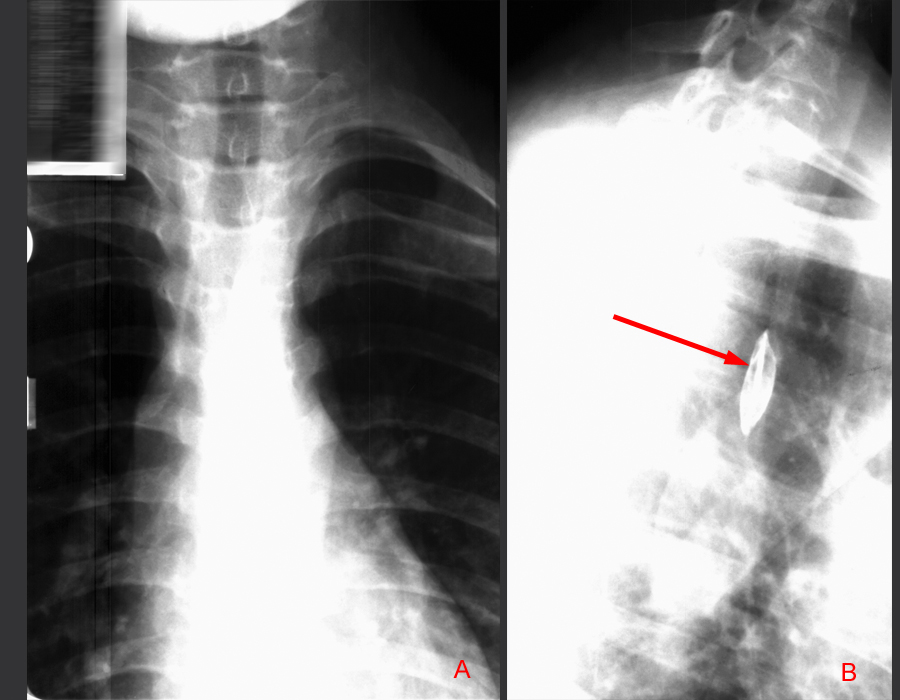
Radiological findings On plain films, one
should obtain anteriorposterior and lateral films of the neck and chest
if foreign body impaction is suspected. Occasionally, the foreign object
may be radiopaque and visualized. Contrast studies can also be performed.
Animal/fish bones may be obscured by barium, but they can sometimes be
visualized as linear filling defects.
Image "A" depicts a frontal view of the chest with no obvious esophageal abnormalities. In the same patient, image "B" shows the lateral view with a barium soaked cotton pledget impaled on a 2.5cm fishbone.
Treatment Foreign bodies can
often be removed via endoscopy or the use of a wire basket or Foley catheter
balloon under fluoroscopic guidance. Non-invasive measures may include
the administration of glucagons with the hopes of relaxing the lower esophageal
sphincter or the use of gas-forming agents to distend the esophagus above
the foreign body to allow passage. |