- Pathogenesis:
- Most likely seen in young women (3%).
- Pathologically, is a non-capsulated
nodular mass:
- Was thought to be a vascular/hamartomatous
malformation.
- Is composed of normal hepatocytes,
Kupffer cells, and bile ducts but arranged abnormally.
- Is less than 5 cm in diameter, most
commonly found peripherally in the right lobe.
- Classic appearance: solitary,
well-circumscribed mass with a central stellate scar of fibrosis even
though the central scar is seen in only 20% of the cases.
- Radiographic findings:
- U/S: the appearance of the lesion is
variable, but low echoes in the center may be seen.
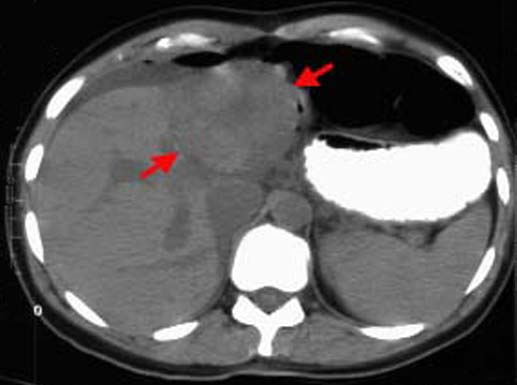
- Noncontrast CT: the lesion has low
attenuation (arrows) compared with the normal liver. The central stellate scar
may also show low attenuation.
- Contrast CT: the lesion shows
homogeneous enhancement early in arterial phase (arrows) with prompt wash-out.
The central stellate scar will not enhance.

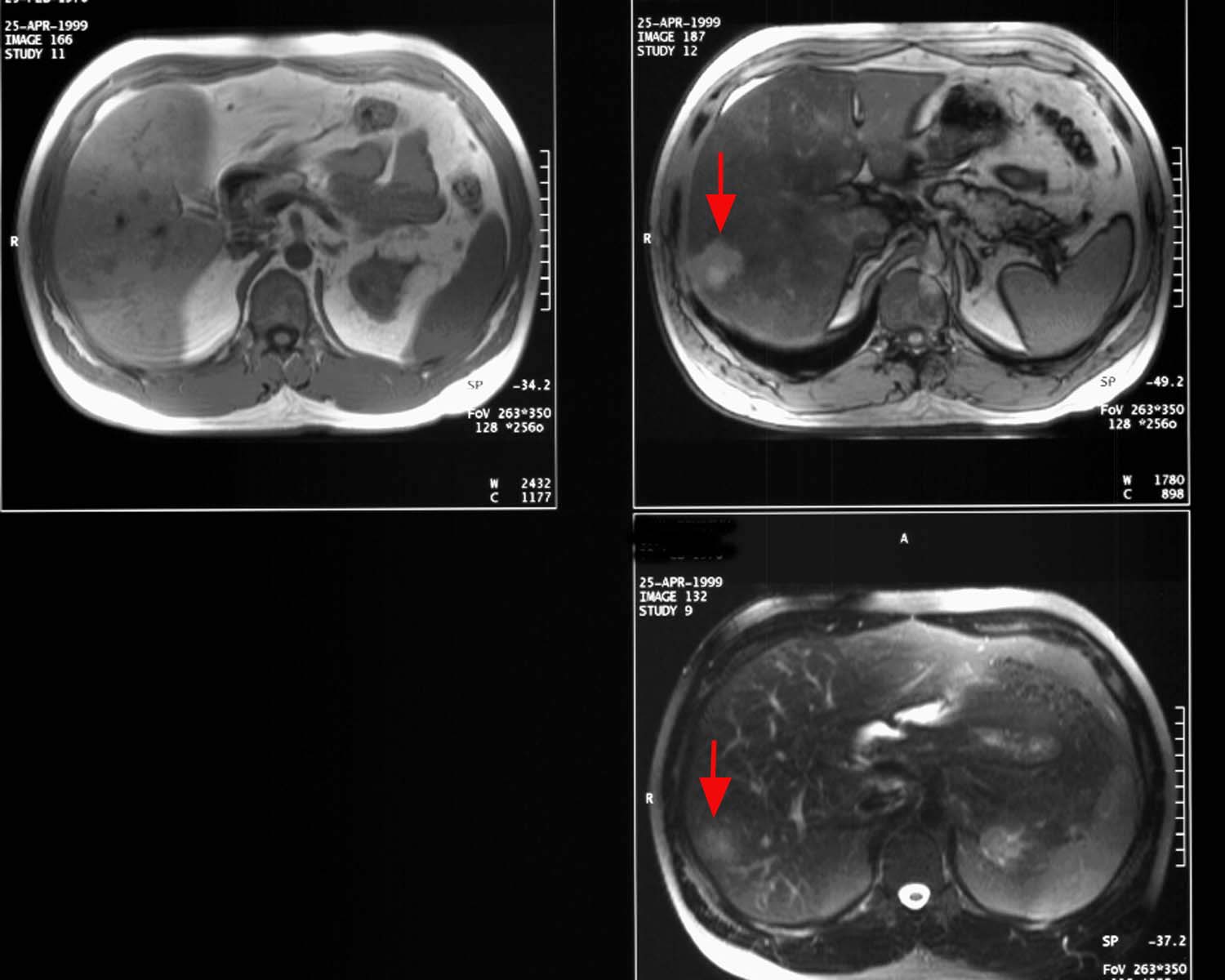
- T1-weighted MRI: the lesion is hypo-isointense
to the normal liver. The central scar enhances with Gd-DTPA.
- T2-weighted MRI: the lesion is
isointense to slightly hyperintense to liver. The central scar is
hyperintense to the liver (arrows) (in contrast to hypointense appearance of
the central scar in large hemangioma).
- Nuclear medicine: sulfur colloid scans
are normal in 50%, have focal photopenic defect in 40%, or focal area of
increased activity in 10%.
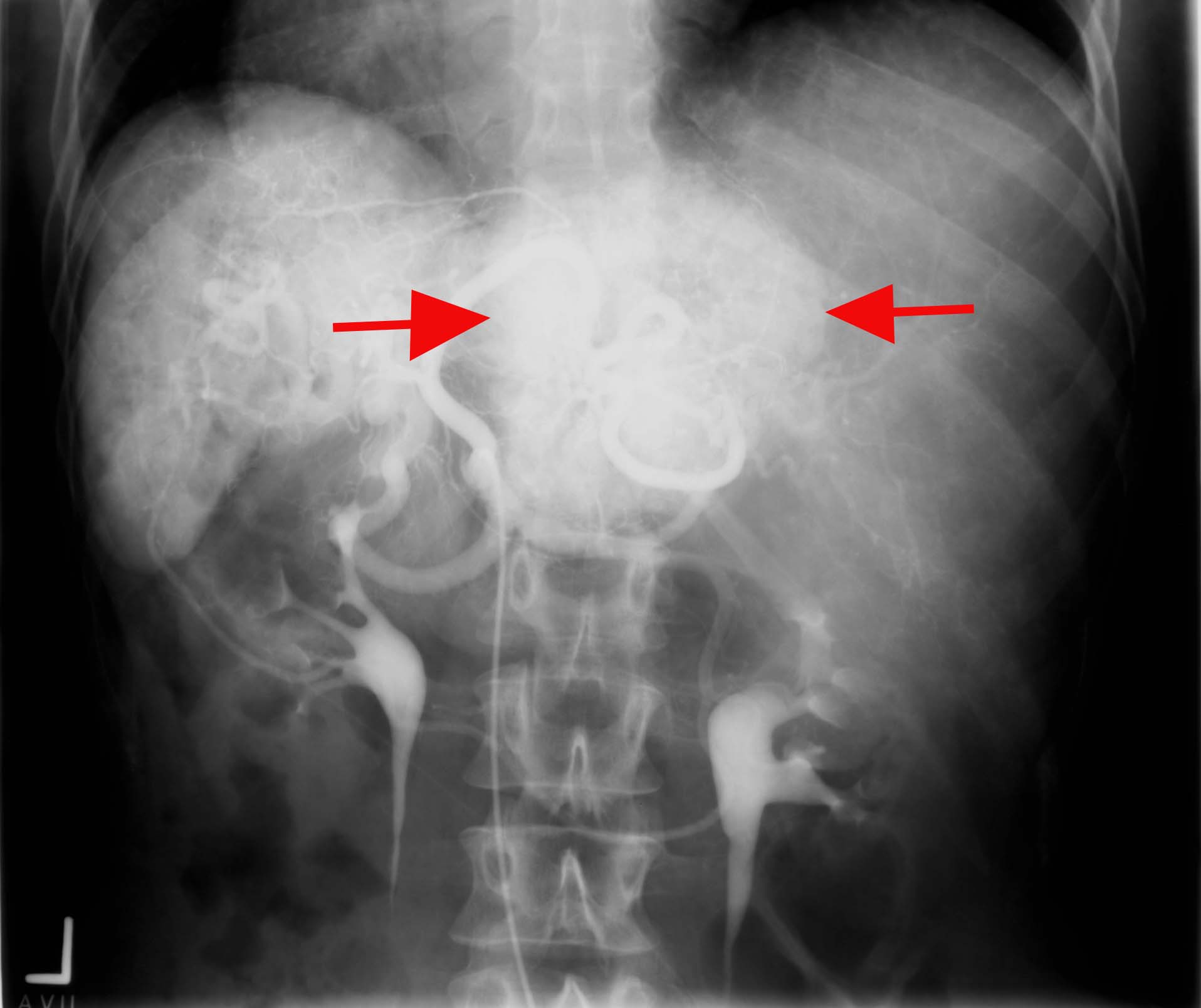
- Angiography: classically shows a
"spoke-wheel" pattern of increased vascularity (arrows).
|