- Pathogenesis:
- Seen in 7% of adults.
- Hemangioma is a benign proliferation of
vascular tissue, lined with endothelium, which has slow hepatic arterial
blood flow. Two types: capillary or cavernous. The former is more
common.
- Uncommon in cirrhosis. Usually
asymptomatic.
- Occurs in the right lobe.
- Can easily be confused with metastases
or hepatoma.
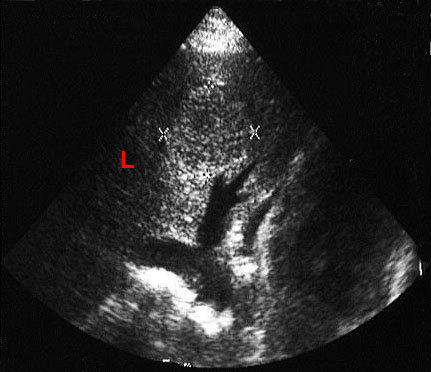
- The most common cause of a hyperechoic
liver mass on U/S.
- Large hemangioma may appear
heterogeneous. There may be thrombosis, or a central stellate scar with
a giant hemangioma.
- Radiographic findings:
- U/S: Hyperechoic and well defined.
- Noncontrast CT: Low attenuation (dark).
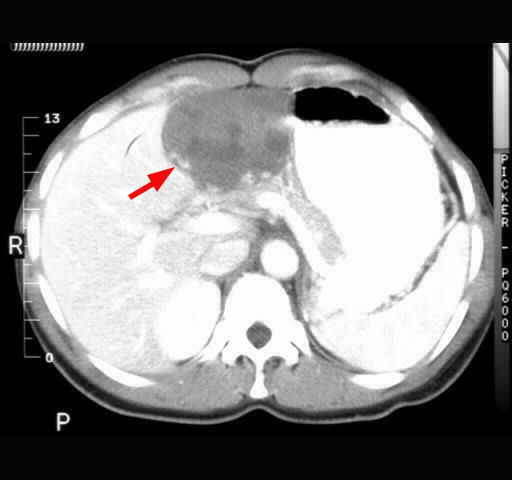
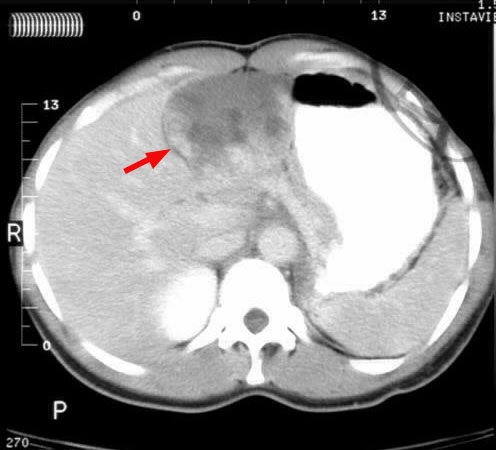
- Contrast CT: Focal nodular enhancement.
80% of hemangiomas have centripetal opacification pattern on delayed CT:
the periphery of the lesion enhances during the arterial phase, the
center fills in (arrows) during the equilibrium phase or early delayed phase. In large hemangioma, the central scar may not enhance due to necrosis.


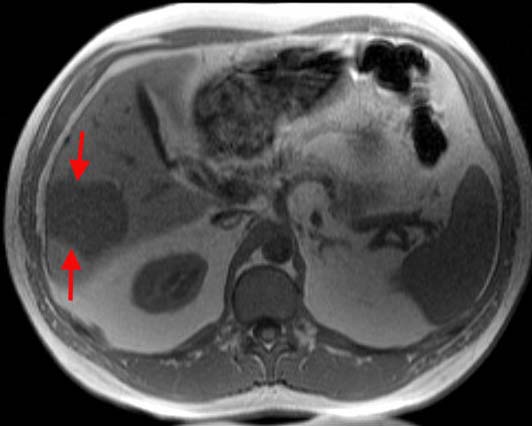
- T1-weighted MRI: Hypointense to liver (arrows).
If gadolinium-diethylenetriamine penta-acetic acid (Gd-DTPA) is used,
peripheral enhancement is seen initially with central enhancement
within 15-30 mins. Enhancement is persistent.
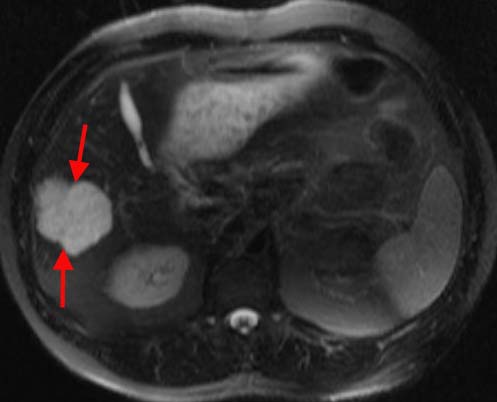
- T2-weighted MRI: Hyperintense to the
liver (just like a cyst; arrows). Looks as bright as a light bulb! Intensity is
as high as that of pure fluid (CSF or bile).
- Gradient Echo: Low signal intensity in
MPGRE (looks completely black).
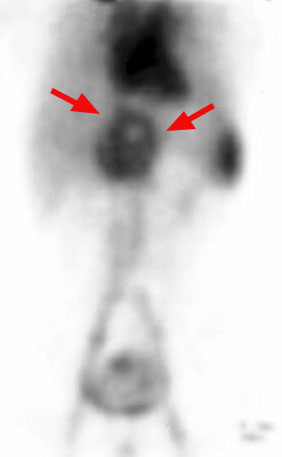
- Nuclear medicine: Lesion fills in on RBC
scan (arrows). Useful for diagnosing hemangiomas > 2 cm in diameter.
|