- Pathogenesis:
- The most common liver masses.
- May be solitary or multiple.
- Cysts are found in 2-10% of population,
has increased frequency with age, and is more common in females aged
50-70.
- True hepatic cysts have bile duct origin
and cuboidal epithelial lining. They are idiopathic, usually asymptomatic, and
variable in size. They cannot be distinguished from cysts that arise
from prior hematomas or abscesses.
- They can be associated with other
disease processes, such as tuberous sclerosis and polycystic kidney
disease.
- ~40% of patients with polycystic kidney
disease have liver cysts. ~ 60% of patients with multiple liver cysts
have polycystic kidney disease.
- Radiographic findings of a simple
hepatic cyst (arrows):
- U/S (95-99% accurate): a. Anechoic, b.
Posterior acoustic enhancement (increased transmitted sound), c.
Well-defined or imperceptible walls.

- Noncontrast CT: density of less than 20
HU, well-defined margins, no perceptible wall (arrow).
- Contrast CT: no enhancement after
contrast administration.
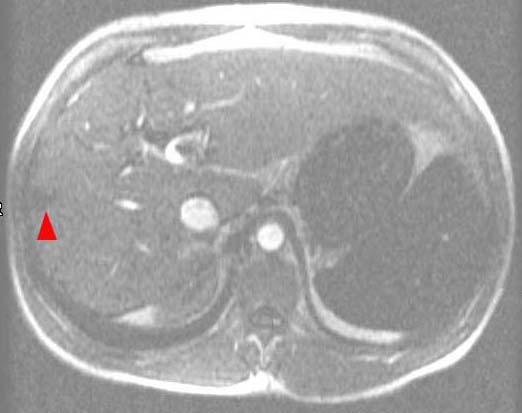
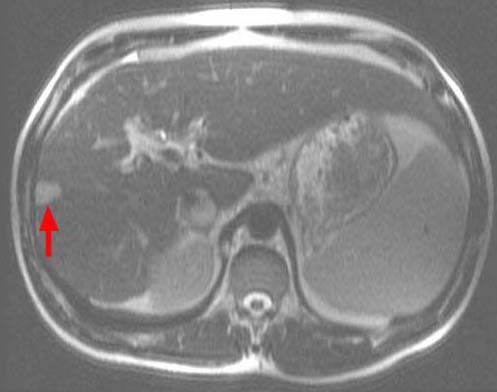
- MRI: a. T1-weighted: homogeneously
hypointense (arrowhead); b. T2-weighted: homogeneously hyperintense (arrow) due to water property (comparable to the intensity of CSF or gall-bladder bile).
Note: cysts can be confused with
hemangiomas on T2-weighted MRI. However, on T1-weighted with
Gd-DTPA, cysts do not enhance whereas hemangiomas do in a centripetal
manner.
A B
- Differential diagnoses of a
cystic liver mass with internal echoes, thick septations, or a
perceptible wall noted on U/S include:
- Hemorrhagic cyst
- Abscess
- Echinococcal cyst
- Biliary cystadenoma
- Cystic metastasis (e.g. ovarian)
- HCC with necrosis
|