- Pathogenesis:
- Incidence of HCC has doubled during the
past 20 years.
- Typically, occurs in an abnormal liver.
Rare de novo development of HCC.
- Risk factors include:
- Cirrhosis of any cause. 80 % of HCC arise in cirrhosis. Cirrhosis from
hepatitis B and/or C has the highest risk for HCC.
- Hemochromatosis
- Steroid use
- Hepatitis B or C infection
- Liver fluke infestation (especially in
southeast asia)
- A typical progression: Cirrhosis--Regenerating nodules--Dysplasia--HCC.
- HCC can be single (50%), multiple (40%),
or diffuse (10%). Often accompanied by hemorrhage and necrosis.
- HCC tends to invade the portal and
hepatic veins and may cause thrombosis.
- HCC can also calcify. Three other
causes of a calcified liver mass include: (1) granulomatous disease, (2)
Metastasis from the colon or stomach, (3) hematoma.
- 85% 4 yr survival if limited disease.
- 25% eligible for surgery provided that
the size of the lesion and its vascular involvement, possible mets, and
advanced cirrhosis are all considered.
- Resection has 5 yr recurrence rate of
80% and 5 yr survival of 30-60%.
- Radiographic findings:
- Noncontrast CT: hypodense; calcification
may be seen.
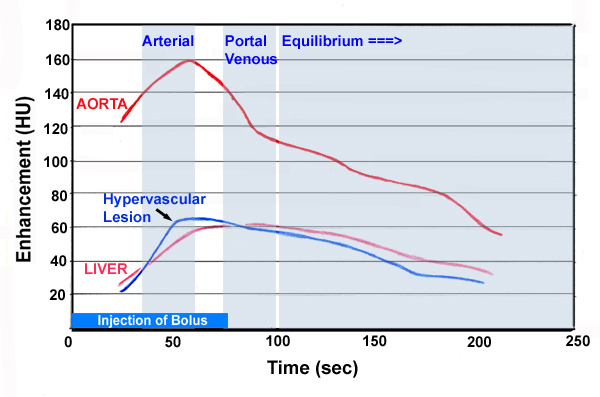
- Contrast CT: dense, diffuse non-uniform
enhancement in arterial phase; some lesions are hypervascular.

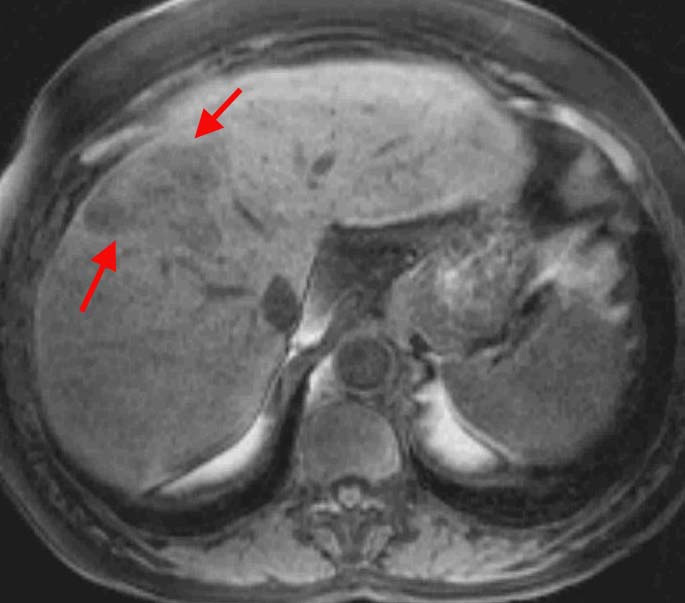
- T1-weighted MRI: usually hypointense to
normal liver. When fatty change, fibrosis, or copper is present,
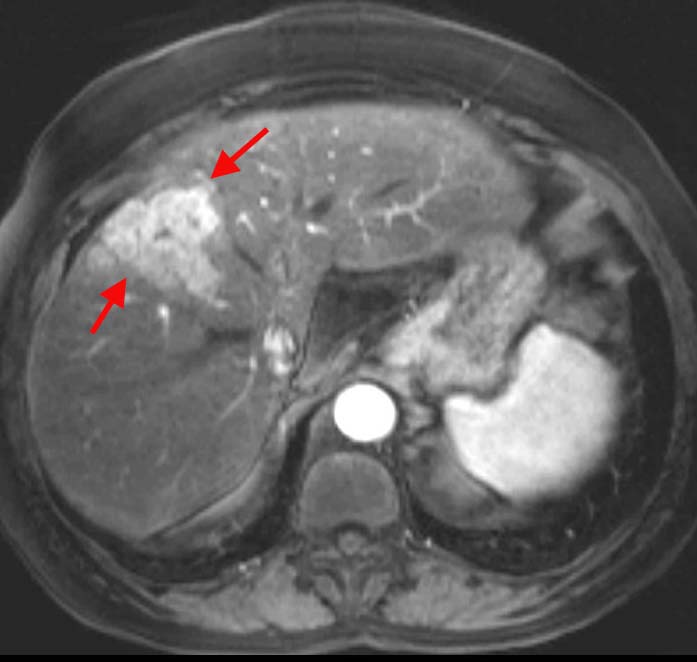
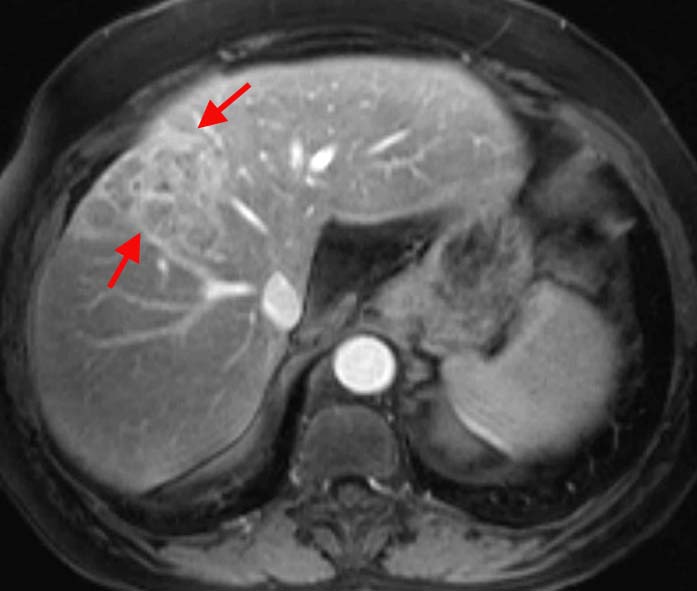
variable signal can be seen. With
Gd-DTPA, hypervascular lesions enhance early in the arterial phase. (Noncontrast on left; arterial phase middle; late venous phase on right.)
- T2-weighted MRI: typically hyperintense
to liver but can be variable. If hemochromatosis is present, the lesion
may appear hypointense. A pseudocapsule may be seen.
- MRA: can be used to assess the patency
of the portal vein and IVC.
- Screening for HCC in cirrhotic
patients:
- Triphasic CT shows 82% of lesions > 2 cm
in diameter and 60% of lesions < 2 cm in diameter (Lim et al AJR 2000).
- Ultrasound can detect 67% of HCC > 3cm
and 12% of HCCs < 3 cm (Bennett et al AJR 2002).
- MRI can detect 80% of lesions >2 cm and
47% of lesions < 2 cm (Krinsky et al Radiology 2001).
|