GI Radiology > Pancreas > Inflammatory > Pancreatitis
Pancreatitis
![]()
|
US, CT, MRCP, and ERCP are all used in the diagnosis and evaluation
of inflammatory diseases of the pancreas. Acute and chronic
pancreatitis, pancreatic abcesses, and pancreatic pseudocysts will be
discussed in this tutorial. The role of diagnostic imaging in acute pancreatitis is quite different from its role in chronic pancreatitis. In cases of suspected pancreatitis, imaging is used to establish an etiology (gallstones, etc), and assess for possible complications that would require intervention. In chronic pancreatitis, imaging allows for the classification of the morphological changes, which determines prognosis and potential interventions. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Acute Pancreatitis:
Common causes of pancreatitis include alcohol abuse, choledolithiasis, hypertriglyceridemia, and hypercalcemia. Acute pancreatitis usually presents as an acute episode of upper abdominal pain, with or without accompanying GI symptoms. Other symptoms may include fever, hypotension, pulmonary edema, or shock. Laboratory values reveal elevated WBC, serum amylase, and pancreatic lipase. Initial treatment of pancreatitis includes NPO, NG suction, analgesics, and parenteral or jejunal feeding. Prophylactic antibiotics may also be of benefit. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Initial evaluation of acute pancreatitis includes an assessment for possible gallstones, and prognostic scoring. A total of 85% of patient with acute pancreatitis (with or without gallstones) will run a benign course and only require supportive measures. The remaining 15% of patients will have a complicated course, which can be predicted using Ranson's criteria (among others). Ranson's score estimates the risk of life threatening complications or death in patients with acute pancreatitis using several factors at the time of admission and during the first 48 hours thereafter. Balthazar et al developed a classification system for patients with acute pancreatitis based on radiologic findings. Both grading systems are summarized below. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
A common complications of pancreatitis is infection; 80% of deaths in cases of acute pancreatitis are due to sepsis. Infection is found in 10% of patients with acute pancreatitis, while it is present in 30-40% of patients with acute pancreatitis complicated by necrotizing pancreatitis. Gram negative rods (E. Coli) are the major culprit. |
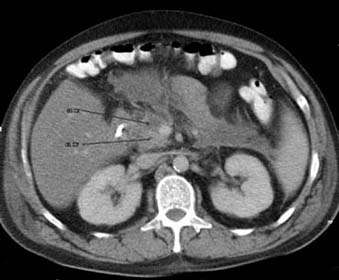
Imaging: Imaging studies performed on admission focus on identifying the cause of the acute pancreatitis. Plain films may reveal secondary effects of acute pancreatitis, including duodenal ileus, jejunal ileus, colon cut-off sign, thickening of the wall of the transverse colon, abnormal separation of the distal stomach from the transverse colon, and left pleural effusion or elevated left diaphragm. Ultrasound is a good diagnostic tool for initial evaluation for gallstones or sludge; US would reveal echogenic gallstones and/or biliary dilation. Contrast enhanced CT (CECT) of the abdomen/pelvis is the imaging standard for evaluating acute pancreatitis. Both intravenous and oral contrast are administered, and thin sections are obtained during the peak of pancreatic arterial perfusion (~30-40 sec post contrast administration). CT findings in acute pancreatitis include focal or diffuse enlargement of the pancreas, heterogeneous enhancement of the gland, irregular or shaggy contour of the pancreatic margins, blurring of peripancreatic fat planes with streaky soft tissue stranding densities, thickening of fascial planes, and the presence of intra- or retroperitoneal fluid collections. Complications of acute pancreatitis may also be present on CECT: pseudocysts, abcesses, necrosis, venous thrombosis, pseudoaneurysms, and hemorrhage. Patients with cholestasis and cholelithiasis/choledolithiasis should also undergo ERCP and endoscopic sphincterotomy (EST) within 72 hours; postponement increases the difficulty of the procedure secondary to duodenal edema. ERCP signs of acute pancreatitis include straightening of the duct secondary to gland edema. Contrast material may also extravasate into the the parenchyma or pseudocyst secondary to autodigestion. Other ductal changes in acute pancreatitis are similar to those of chronic pancreatitis, although less dramatic changes would be expected. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Studies have also shown that ERCP and EST treatment of acute biliary pancreatitis
(with stones in the distal bile duct) reduced morbidity and mortality. Other studies have even
demonstrated the benefits of ERCP and EST in the absence of visualized
stones. The absence of gallstones on ERCP does not exclude gallstone
disease as an acute etiology, especially in cases of biliary
microlithiasis. Some data suggest that ERCP and EST may be indicated in
all patients with acute pancreatitis who have a prognostically severe
pancreatitis according to Ranson's criteria (unless alcohol is a very
likely etiology). The prognosis for these patients varies from uneventful recovery to deterioration with pancreatic necrosis, abscess, or pseudocyst formation. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||