GI Radiology > Pancreas > Inflammatory > Pancreatitis
Pancreatitis
![]()
|
Chronic
Pancreatitis:
Chronic pancreatitis presents with different diagnostic and therapeutic challenges compared to acute pancreatitis; the role of imaging may be interventional as well as diagnostic. Chronic pancreatitis is characterized by parenchymal atrophy, ductal calcifications, and ductal dilatations and strictures. The etiologies of pancreatitis were listed in the previous table. Chronic pancreatitis may present with upper abdominal pain, signs of obstructive jaundice or duodenal obstruction, or exocrine/endocrine dysfunction of the pancreas itself (malabsorption, hyperglycemia). Diagnosis of chronic pancreatitis is usually based on clinical symptoms, detection of endocrine/exocrine insufficiency, and morphological finding on imaging.
Plain Film:
Computed Tomography (CT): |
||||||||||||||||||
|
||||||||||||||||||
|
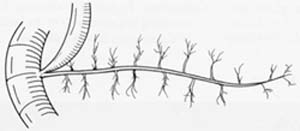
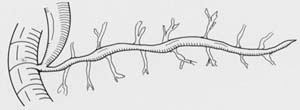
Endoscopic Retrograde Cholangiopancreatography (ERCP): ERCP is considered the most sensitive imaging modality for diagnosing chronic pancreatitis. However, there may be few imaging findings in patients with less advanced disease. ERCP may also be difficult in patients with severe strictures or obstructing stones/calcifications. Furthermore, a normal ERCP does not rule-out pancreatitis, since ERCP may miss microlithiasis. Duct abnormalities such as irregular contours, strictures, dilatation, and opacified pseudocysts are all indicative of chronic pancreatitis, and are listed in the following table. |
||||||||||||||||||
|
||||||||||||||||||
|
Several classifications systems have been developed for the evaluation of chronic pancreatitis. The table below demonstrates one such system. |
||||||||||||||||||
|
||||||||||||||||||
|
Bile duct changes secondary to chronic pancreatitis may be demonstrated
on ERCP. The following table summarizes bile duct findings on ERCP
in chronic pancreatitis. |
||||||||||||||||||
|
||||||||||||||||||
|
Magnetic Resonance Cholangiopancreatography (MRCP): |
||||||||||||||||||
|
Interventional radiology: |
||||||||||||||||||