Pseudocysts occur most frequently in patients with acute or
chronic pancreatitis; other etiologies include pancreatic trauma,
pancreatic ductal obstruction, or neoplasm. Following an episode of pancreatitis, pancreatic
enzymes cause local inflammation and tissue distruction. This process
causes exudation of fluid from the pancreas which collects within the
pancreatic membrane or the surrounding compartments. Most of these
"acute fluid collections" resolve
within 4-6 weeks; if these collection persists, it evolves into a pseudocysts with
a fibrotic capsule. (It should be noted that the capsule of a
pancreatic pseudocyst does not have a true epithelial lining, which
distinguishes it from a cystic pancreatic neoplasm.) Most
pseudocysts are located in the lesser peritoneal sac, near the pancreas.
Larger pseudocysts can extend into the paracolic gutters, pelvis, and
mediastinum.
Pseudocyst development should be suspected in patients with
persistant abdominal pain, mild fevers, and elevated amylase or lipase,
following resolution of pancreatitis. Complications of pseudocysts
include infection (most common), obstruction, perforation, hemorrhage
(eroding adjacent vessels).
US and CT can detect pseudocysts as small as 5 mm.
Opacification of the ducts during ERCP may also
assist in the visualization of pseudocysts by highlighting secondary
signs of ductal obstruction or displacement. Furthermore, 30-80% of
pseudocysts communicate with the pancreatic duct, and become visible
during fluoroscopy. Care must be taken to prevent over distention of the pseudocyst
during ERCP, and patients must be monitored for signs of sepsis
after the
introduction of contrast medium into the cyst. |
|
Pseudocyst
Findings |
|
 |
Contrast-enhanced CT:
-Low attentuation and homogenous appearence
-Well-defined, nonepithelial, fibrous wall (distinguished this from
actue fluid collection)
-Round or ovoid shape |
|
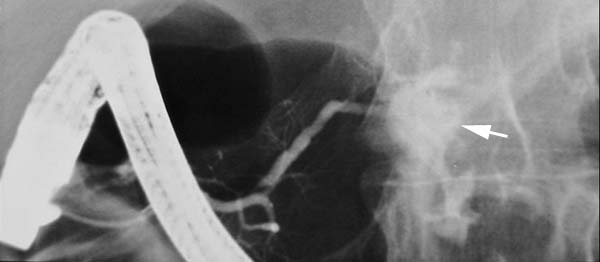 |
ERCP:
-Communicating pseudocyst filling with contrast. |
|
The table below distinguished the radiographic findings of
pseudocysts and acute fluid collections:
|
Distinguishing Radiographic
Features of
Pseudocyst vs. Acute Fluid Collection |
|
Pseudocyst |
Acute
fluid collection |
|
|
 |
-Round, ovoid,
well-defined
-Well-defined, fibrous wall |
-Poorly defined shape
-No fibrotic capsule |
|
|
Weekly U/S are recommended to monitor the evolution of pseudocysts,
should one be discovered in the workup of pancreatitis.
A small fluid
collection within the first 6 weeks may be tolerated and evaluated for
progression. Pseudocysts > 5cm, growing, or persistent for more than 6
weeks, should be treated regardless of the presence of symptoms. US or
CT guided drainage is advised for such cases; surgical intervention is
rarely indicated because of the development of endoscopic and interventional
radiological procedures. |
|
|