PostOperative Cholangiography (cont.)

Procedure
(cont.)
|
- After the connection is made, the clamps
are removed from both tubes. Gentle aspiration of the syringe will reveal
whether or not there is an air bubble present at the connection. If
so, the tubes must be reclamped, the connection separated, and the bubbles
expelled before reconnecting. This procedure is repeated until no air
bubbles can be identified at the connection of the t-tube to the extension
tubing. (Air bubbles in the bile ducts look exactly like retained stones.)
- The patient is rotated into a steep LPO (nearly left lateral)
position and the fluoroscopic table is tilted about 30° head down. In
this position, the left lobe of the liver is dependent, and the left
intrahepatic ducts will fill by gravity. Also, in this position, the
confluence of the right and left hepatic ducts is optimally demonstrated
without overlap.
- The water-soluble contrast agent is slowly
injected by hand while duct filling is monitored by fluoroscopy. When
the branching ducts in the left lobe of the liver have filled and the
right hepatic ducts begin to fill, take the first spot image(s) (2-on-1
format, 109 kVp).
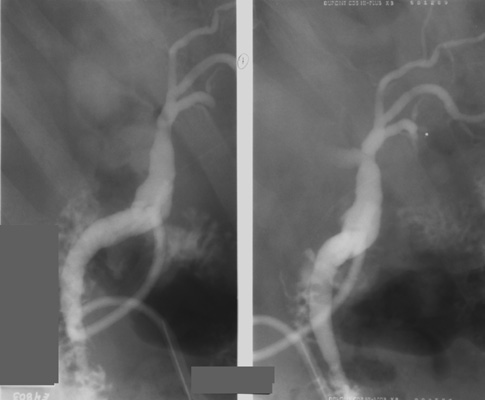
- Roll the patient to the supine position
and continue filling the ducts until the branches in the right lobe
are filled along with the extrahepatic duct. Again, take a spot image(s)
(2-on-1 format, 109 kVp). Try to time the exposure for when contrast
squirts from the common bile duct (CBD) into the duodenum.

|
|
|

