Anal canal.
-
The anal canal should remain closed in the resting state
and with each maneuver other than defecation.
-
An open anal canal should be subjectively reported as being
slightly or widely open.
-
Incontinence of barium/stool at any time is abnormal.
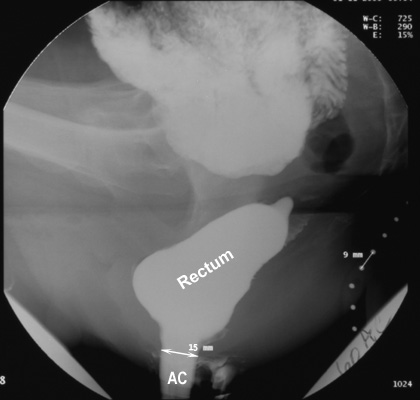
- The anal canal length is measured as the distance
between the external anal orifice and the point where the parallel
straight sides of the anal canal meet the cone-shaped walls of the distal
rectum. The mean radiographic length of the anal canal in men is 22 mm and
in women, 1.6 cm. During evacuation, the width of the anal canal averages
15 mm and seldom exceeds 2 cm.
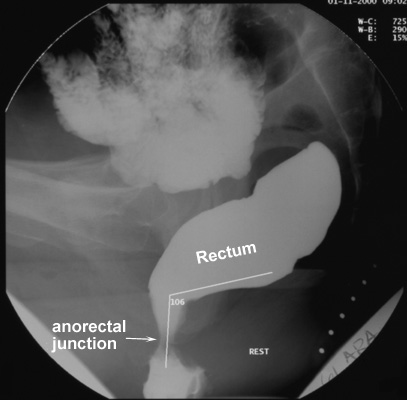
Anorectal junction position
- The site of the anorectal junction is the point where
the parallel straight sides of the anal canal convert to the diverging
walls of the distal rectum.
- This point is measured with reference to the
inferior margins of the ischial tuberosities.
- In young subjects, the anorectal junction lies close to this bony landmark.
- During maximal
straining, the anorectal junction should descend a distance of no more
than 3.5 cm from its resting position.
- The movement of the anorectal junction during "squeeze"
and defecation are calculated as follows:
- Perineal elevation =
"squeeze" value - resting value
- Perineal descent = resting
value - defecation value
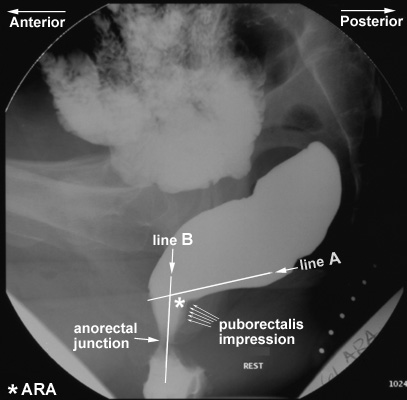
Anorectal angle (ARA)
- The puborectalis muscle, a component of the levator ani
muscle group, originates from one pubic bone, extends posteriorly around
the anorectal junction, and passes anteriorly again to attach to the other
side of the pubis. Thus, it forms a sling around the anorectal junction
and produces a posterior indentation on it.
- It is believed that fecal
continence depends not only on the intrinsic anal musculature but also on
a flap-valve effect produced by the puborectalis sling. This muscle is
tonic at rest and produces an angle of about 90° between the anal canal
and the lower rectum.
- The anorectal angle or
ARA (demonstrated by *
in the image below) is the angle
between a
line drawn parallel to the posterior wall of the rectal ampulla just above
the impression of the puborectalis sling (line A in the image below) and a line drawn in the axis of the anal canal (line
B in the image below).
- Changes in the ARA are representative of the activity of the
puborectalis muscle.
- Change in the ARA is measured during "squeeze" and
defecation with reference to the resting value.
- The ARA normally decreases
(becomes more acute) during squeezing, indicating contraction of the
pelvic floor musculature.
- The ARA normally increases (becomes more obtuse) when
the subject strains down to defecate, due to relaxation of the puborectalis muscle and loss of its posterior impression on the anorectal
junction. The range of normal ARA measurements is very wide (see
the table on the next page).
Rectosigmoid gap
- Normally, the retrorectal (presacral) space is <1 cm wide.
- If the rectum is
poorly fixed to the sacrum and a posterior cul-de-sac is present, the
patient is predisposed to rectal prolapse. This condition is indicated by
a widened recto-sacral gap of >1 cm.
|