Rectal Intussusception And Prolapse
-
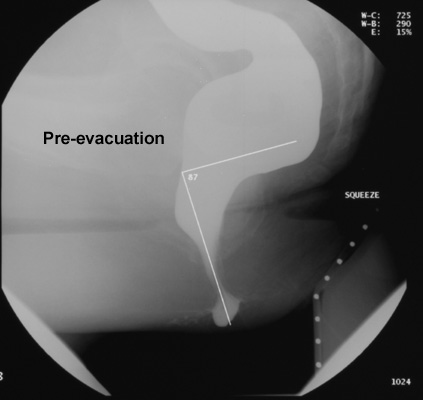
Rectal intussusception is an abnormal condition in which the proximal
rectal wall invaginates into the distal rectum during defecation and
persists after the bolus has passed.
-
When the lead point of the intussusceptum passes beyond the external anal orifice, the condition is
designated rectal prolapse.
-
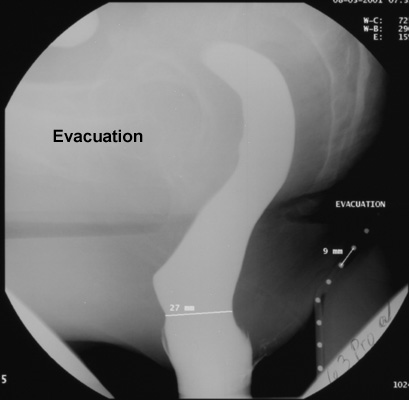
During downward straining, the intussusceptum
occludes the anal canal, preventing further evacuation of rectal contents.
The most common symptoms are constipation, incomplete emptying, rectal
bleeding, perineal pain or pressure, and fecal incontinence. However, mild
mucosal intussusception may also occur in subjects without anorectal
symptoms.

-
Rectal intussusception has three stages of severity:
- Stage I, rectal intussusception: A mucosal fold develops in the
rectal wall and gradually deepens to form an intussusception of the full
thickness of the rectal wall into the rectal lumen. However, a minimal
infolding that disappears after the bolus has passed is probably caused
by transient invagination of the rectal mucosa and should not be considered
pathologic.
- Stage II, intraanal rectal intussusception: The apex of the rectal
intussusceptum passes down into the anal canal.
- Stage III, rectal prolapse: The intussusception passes through the
anal canal and protrudes externally. It is termed a complete external
rectal prolapse when the entire thickness of the rectal wall protrudes
beyond the anus. Partial prolapse is the designation when the protrusion
consists of mucosa only.
- In some patients, this process develops gradually and slowly so that it
is easy to recognize. In others, the rectal wall prolapses suddenly, only
at the end of rectal evacuation, so that it is necessary to ask the
patient to evacuate as completely as possible during the examination.
- Most
intussusceptions originate from the anterior wall (60%) or begin in an
annular fashion (30%). The posterior wall is rarely the origin. Intussusception most often develops at the level of a valve of Houston,
approximately 6-8 cm from the anal margin.
- All patients with an
intussusception have a concomitant rectocele. In patients who develop
external rectal prolapse, the rectum assumes a vertical axis and is
displaced away from the curve of the sacrum when the patient is straining.
- The anatomical prerequisite for a rectal intussusception to occur is that
the proximal rectum is an intraperitoneal organ. In such cases, the normal
retroperitoneal position is changed, and there is a mesorectum present.
The abnormal attachment of the rectum may or may not be accompanied by a
deep pouch of Douglas.
|