- The patient remains in the left lateral
position.
- Unclamp the tubing and allow barium to flow by gravity or by
gently squeezing the enema bag.
- When you estimate that the rectum is
filled with barium, check the position of the enema tip with fluoroscopy
and inflate the retention balloon in the rectal ampulla with only
one puff of air during fluoroscopic monitoring.
- You can
avoid causing rectal discomfort and urgency throughout the examination by
only half filling the balloon.
- Understand that the purpose of the balloon is to keep the enema tip from coming out - not to block egress
of barium.
NOTE: Do not inflate the
retention balloon in the presence of a large rectal tumor, acute
inflammation, stricture, or recent biopsy because of the potential for
rectal perforation.
NOTE: No further
fluoroscopy is ordinarily necessary until Step #4, below.
- As the barium continues to flow, tilt head of x-ray
table down about 15 degrees. When the bag is empty of barium, clamp the tubing,
and return the table to a horizontal position.
-
Begin insufflating air at a rate of not
more than one puff per second. Add 5 puffs of air in each of the
following 9 patient positions: left lateral, LAO, prone, RAO, right
lateral, RPO, supine, left lateral, and, finally, prone.
- After the final turn and air insufflation, look to see that barium has entered the ascending colon. If
barium is in the ascending colon, proceed to Step #5. If not, perform
Modification #1, to be followed by Modification #2, if necessary (see
Modifications, below).
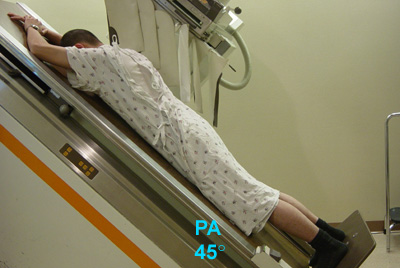
-
With the patient in the prone position, raise the
head of the table 45°. Place the barium bag between the patient's
legs, unclamp the tubing, and allow barium to drain from the rectosigmoid.
|