GI Radiology > Small Bowel > Neoplasms > GIST
Neoplasms
![]()
Gastrointestinal Stromal Tumor (GIST) |
|
GIST are primary
gastrointestinal tumors of mesenchymal origin that develop in the muscular
layer of the intestinal wall. GIST
encompasses several tumors of varying differentiation, incuding leiomyomas
and leiomyosarcomas. These tumors comprise less than 3% of primary GI
neaplasms and ~10-15% of small bowel malignancies. The small bowel is the
most common site for GIST. Size can range from a few millimeters to greater
than 30-40 centimeters. Large
GIST often outgrow their blood supply, leading to necrosis and hemorrhage.
GIST vary widely in their malignant potential, and size is a poor predictor
of malignant potential. Instead,
malignancy is based on histological findings (number of mitoses per HPF) and
metastasis. The tumors usually spread through local growth, with metastases
usually involving the liver and/or peritoneum. Local recurrence after surgical excision is extremely
common for both benign and malignant neoplasms. Local growth can occur
exophytically or intraluminally.
Intraluminal growth usually preserves the mucosal layer of the
intestine, unless tumor necrosis causes ulceration. Signs and symptoms are variable. Large local growth can lead to abdominal masses, abdominal pain, and intestinal obstruction. The predisposition to necrosis and hemorrhage can lead to GI bleeding and perforation. Treatment has historically been surgical excision, with leiomyosarcomas carrying a 30% 5-year survival rate. |
|
Leiomyoma. Gross pathology demonstrates a well-circumscribed homogeneous mass protruding into the mucosa of the small intestine. |
RadiologicalPlain films are often
normal in GIST, but may demonstrate an obstructive pattern or perforation. Fluoroscopy
will demonstrate a filling defect.
The angles at the margins of GIST are usually obtuse, evincing the
intramural nature of the tumor.
The mucosa is preserved unless ulceration occurs. In such cases, the lesion may take on
a bull’s-eye appearance, with contrast filling the necrotic tumor cavity. |
|
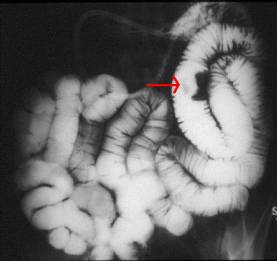
Leiomyoma. Enteroclysis demonstrates a solitary filling defect in the jejunum (red arrow). Note the obtuse angle of the margins, suggesting the intramural location of the mass. |

![]()
![]()