Head CT > The Final Quiz Answers
The Final Quiz Answers
![]()
Question 1: Which of the following is NOT true concerning epidural hematoma?
Question 2: Which of the following is NOT true concerning cerebral contusion?
Question 3: Which of the following is NOT true concerning diffuse axonal
injury?
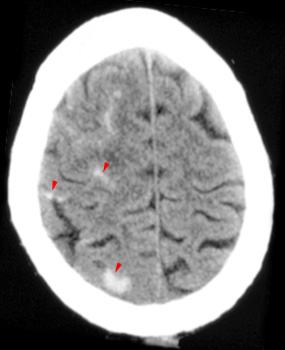
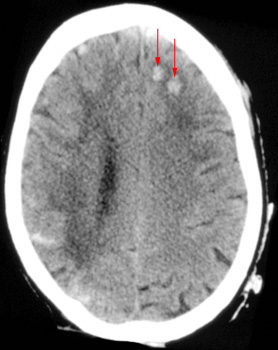
Question 4: Given the following CT, the
most likely diagnosis is:
Question 5: The CT on the left, taken prior
to contrast administration and the CT on the right, taken after contrast
administration, show:
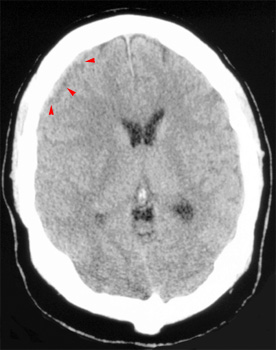
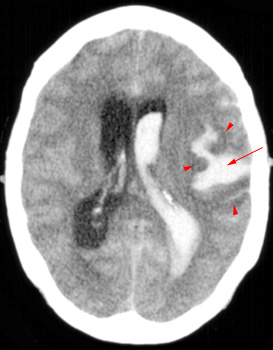
Question 6: Given the following head CT, the most likely diagnosis is:
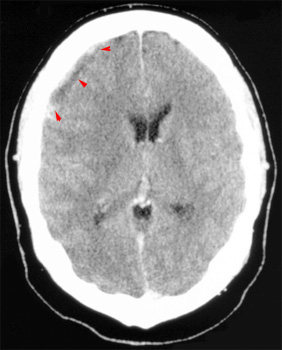
Question 7: Given the following head CT, the most likely diagnosis is:
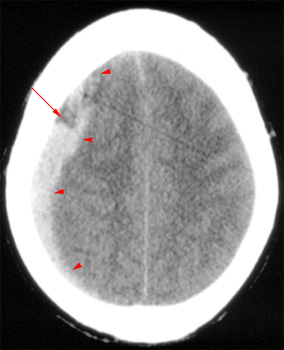
Question 8: Which of the following is NOT shown in this CT?
Question 9: Which of the following is NOT an advantage to performing a CT
scan for stroke?
Question 10: Which of the following is NOT
true concerning CT?
![]()