Surgical Respiratory Neonatal Distress

|
Congenital Cystic Adenomatoid Malformation (CCAM)
Congenital cystic adenomatoid malformation is a hamartoma of the lung. If there is significant mass effect in the chest, CCAM is surgically resected. Occasionally CCAM can regress. CCAM that is discovered on prenatal US may not be recognized on the postnatal CXR. Chest CT may be necessary to demonstrate the CCAM. If the CCAM is asymptomatic then it is uncertain whether surgical resection is necessary. An argument can be made for surgical resection because of reported cases of lung cancer arising from CCAM.
The presentation can vary from a large cystic lesion to a grossly solid appearing lesion that is composed of microscopic cysts. CCAM has a normal pulmonary arterial supply as opposed to pulmonary sequestration. Three types of CCAM are recognized depending on gross appearance:
Type I CCAM - Most frequent (2/3 of cases), contains a dominant cyst > 2 cm surrounded by multiple, smaller cysts.
Type II CCAM - (15-33%) uniform smaller cysts up to 2 cm. Other congenital malformations are associated with Type II CCAM in 50% of cases.
Type III CCAM - Least common (< 10%), contains microscopic cysts that are not grossly visible. Grossly and on imaging the lesion appears solid. Fetal hydrops and maternal polyhydramnios are frequent complications.
|
| | |
 |
 |
|
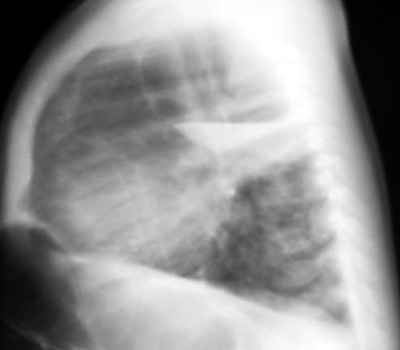
Example of a Type 1 CCAM on CXR with a large dominant cyst
containing an air fluid level
|
| | |
 |
 |
|
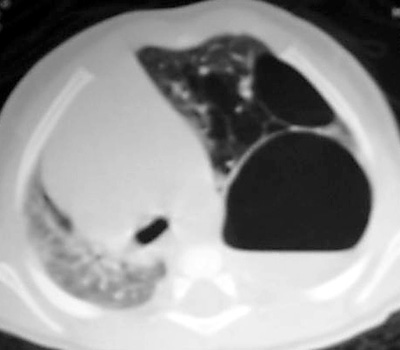
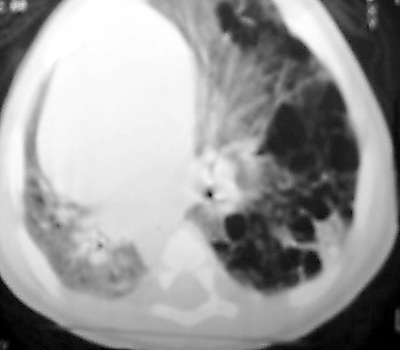
Chest CT on the same patient confirms a Type I CCAM with a large dominant cyst
surrounded by multiple smaller cysts
|
| | |

