Surgical Respiratory Neonatal Distress

|
Congenital Lobar Emphysema (CLE)
Congenital lobar emphysema is characterized by overexpansion of one or more lobes. Emphysema is a misnomer as there is no destruction of alveoli. The etiology of CLE is not entirely clear, but it is thought to result from an airway obstruction, which can arise from a myriad of causes. However, even at surgical resection and pathologic examination, the cause is not usually identified. Prior to resection CT and bronchoscopy are helpful to rule out a treatable cause such as a pulmonary sling.
CLE has a distinct anatomic distribution: 43% in the left upper lobe, 32% in the right middle lobe, and 20% in the right upper lobe. CLE is very uncommon in the lower lobes. Initially, CLE will appear as a solid mass on both prenatal US and postnatal CXR because of the delayed clearance of pulmonary fluid. Over several days the fluid will slowly resorb, and the classic findings of a hyperlucent lobe will be present. The initial appearance of a CLE as a solid chest mass may mimic CCAM, sequestration or even a tumor. The appearance of a CLE as a hyperlucent lobe can be confused with a pneumothorax.
|
| | |
 |
 |
|
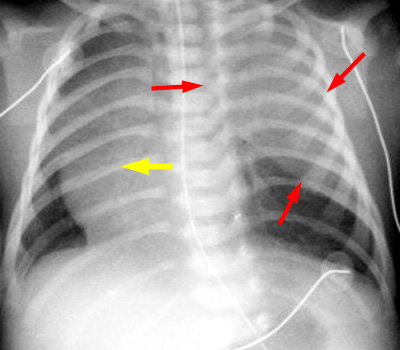
Initial postnatal CXR demonstrates a solid appearing mass in the left upper chest (red arrows) with mass effect and shift of the mediastinum (yellow arrow). At this point, the CLE is filled with fluid and thus mimics a solid mass.
|
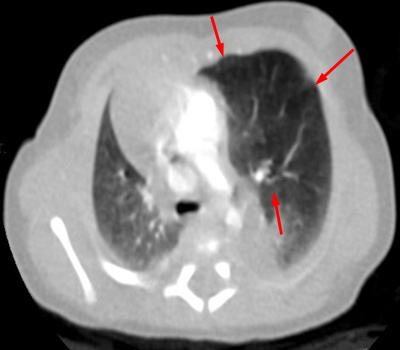
Chest CT on day 2 of life. The fluid has been absorbed and the left upper lobe is shown to be hyperinflated resulting in mass effect and shift of the mediastinum.
|
| | |
 |
|
The gross specimen confirms the hyperexpansion of the left upper lobe.
|
| | |

