Pediatric Radiology > Musculoskeletal > The Pediatric Hip > Developmental Dysplasia of the Hip
Developmental Dysplasia of the Hip
![]()
|
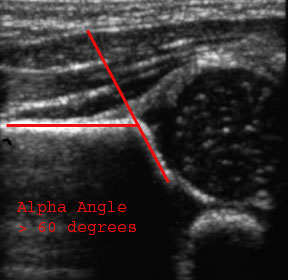
Developmental Dysplasia of the hip (DDH), also known as congenital hip dislocation, is recurrent subluxation or dislocation of the hip secondary to acetabular dysplasia, abnormal ligamentous laxity, or both. The acetabular dysplasia yields an increased acetabular angle and a shallow acetabular fossa. Early diagnosis of DDH is important because chronic dislocation of the femoral head can lead to growth deformity of the acetabular fossa. DDH is much more prevalent in females than males (9:1). It also is predisposed to affect the left hip > right hip (approximately 70-75% of the time). DDH is seen bilaterally in 5% of patients. Clinical findings of DDH include a shortened leg with decreased range of abduction when flexed, asymmetry of the gluteal folds, and positive "clicks" with dislocation (Barlow maneuver) and relocation (Ortolani maneuver). Ultrasound is the study of choice at most centers when clinical suspicion of DDH is present. It allows the hip to be evaluated for both abnormal mobility and dysmorphic acetabular features. Ultrasound is not generally performed in the first two weeks of life due to physiologic ligamentous laxity likely from maternal estrogen effects. Ultrasound is also not generally performed after 6 months of age due to increasing ossification of the femoral head. Plain film radiography has a very limited role in evaluation of DDH in children under 6 months of age due to the lack of ossification of the femoral head. In particular, radiographs are unreliable in children 6-12 months of age because of a lack of skeletal ossification. When radiography is used, AP views are most helpful as frogleg views are likely to reduce a subluxed or dislocated hip.
|
||||||||||
|
|
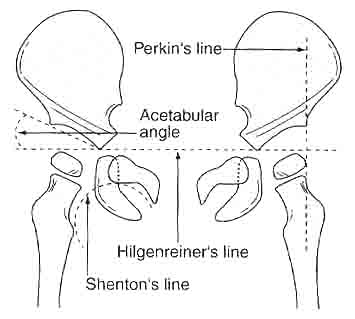
Shenton's curve: smooth, curved line connecting medial border of femoral metaphysis with the superior border of the obturator foramen Hilgenreiner's line: a horizontal line through the triradiate cartilage of the acetabulum Perkin's line: a vertical line (perpendicular to Hilgenreiner's line) from the lateral margin of the ossified acetabular roof that is normally tangential to the lateral margin of the ossification center of the femoral head Acetabular angle: angle that the acetabular line makes with Hilgenreiner's line |
|||||||||


![]()
![]()