Pediatric Radiology > Musculoskeletal > Aggressive Lesions > Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
![]()
|
Langerhans Cell Histiocytosis (LCH), previously known as histiocytosis X, is an idiopathic disease characterized by abnormal proliferation of Langerhans cells. The disease can exist along a spectrum from localized to systemic manifestations. The disease is more common in males > females (2:1), and more prevalent amongst the caucasian population. Radiographic findings are highly variable; bony lesions may be sclerotic or lucent, have a sclerotic or poorly-defined border, and be permeative or geographic in appearance. The most common sites with radiographic findings are: skull > ribs > femur > pelvis > spine > mandible. Classification is controversial but the 3 main clinical subtypes of LCH are: Unifocal, previously known as Eosinophilic Granuloma - most common form with best prognosis; disease isolated to bone or lung; usually presents between 5 and 15 years of age
Multisystem, previously known as Letterer-Sewe disease - acute, diffuse, and often fatal; worst prognosis; usually presents before age 2
Multifocal, previously known as Hand-Schuller-Christian disease - chronic and diffuse with high morbidity; fatal in about 15% of patients; usually presents before age 5
|
|||||
 |
 |
||||
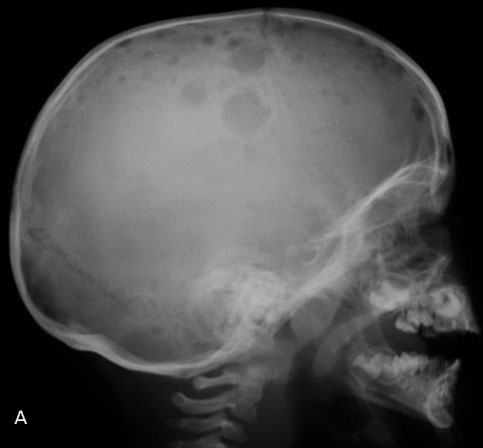
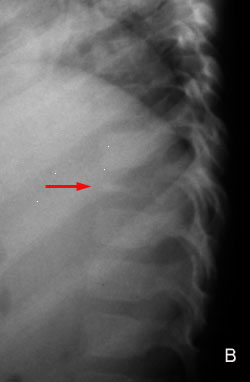

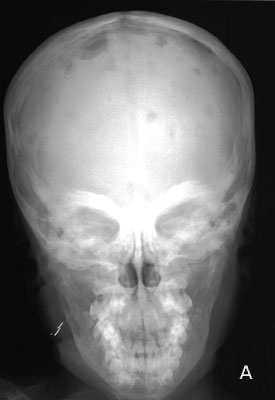
| Langerhans Cell Histiocytosis in a 4-year-old male. A, AP view of the skull demonstrates multiple well-defined lytic lesions. Note the involvement of the right mandible as well. B, AP radiograph of the pelvis shows lytic lesions (arrows) involving the iliac regions and the proximal femurs bilaterally. |
 |
A classic example of "floating teeth" in a child with Eosinophilic Granuloma. Note the bilateral lytic lesions involving the mandible on this panorex view. |
![]()
![]()