Cardiac MRI > Pathology > Disease of the Aorta and Great Vessels > Aortic Dissection
Aortic Dissection
![]()
Aortic dissection is due to the formation of a tear in the intimal layer of the aortic wall, usually as the result of hypertension. Blood flowing under the intimal tear produces a false lumen adjacent to the true lumen of the vessel. Complications of aortic dissection include rupture resulting in internal hemorrhage, propagation of the dissection into the coronary arteries or branches of the aortic arch resulting in vessel occlusion, or rupture into the pericardium causing pericardial tamponade. Dissections that include the ascending aorta and aortic arch proximal to the origin of the left subclavian artery (DeBakey 1 and 2, Stanford A) require surgical treatment while those that only involve the aorta distal to the left subclavian artery (DeBakey 3, Stanford B) can be treated medically with stringent blood pressure control.
MRI is a very accurate technique for assessing aortic dissections, as is CT angiography and transesophogeal echocardiography. MRI is excellent for assessing the extent of the dissection as well as the presence of complications including pericardial effusion and aortic valve pathology. These patients can be critically ill and MRI is not appropriate for unstable patients. Visualization of the intimal flap is crucial to making the diagnosis, and localizing the extent of the dissection is important for determining management and prognosis. Aortic regurgitation may be present, which causes a regurgitant jet on cine imaging.
 |
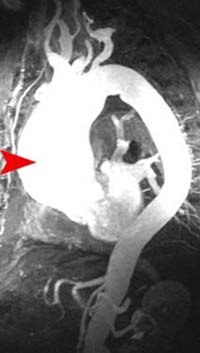 |
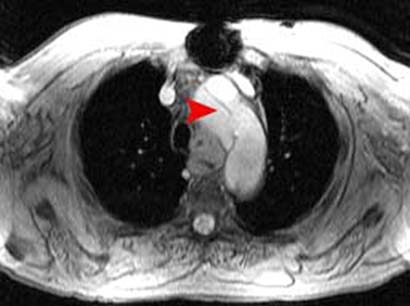
Shown above are an axial image (left) and a maximum intensity projection (MIP) MRA (right) from a patient with an ascending aortic dissection, which would be classified as Stanford Type A. An intimal flap can clearly be seen in the axial image. However, the MIP image shows only the resulting aneurysmal dilation and not the intimal flap, which is a limitation of the technique.
![]()
![]()