Cardiac MRI > Pathology > Cardiomyopathies > Restrictive Cardiomyopathy
Restrictive Cardiomyopathy
![]()
Restrictive Cardiomyopathy (RCM) is another cause of diastolic heart failure. The myocardial wall in RCM is too rigid to allow for relaxation due to fibrosis or infiltration by other tissues. The most common infiltrative causes of RCM include amyloidosis, hemochromatosis, and sarcoidosis. The general cardiac MRI features of RCM include normal LV size and systolic function, diastolic dysfunction, and dilation of both atria. Clinically, RCM is often difficult to differentiate from constrictive pericarditis but Cardiac MRI can help to make this distinction.
Hypereosinophilic endomyocardial fibrosis (Loeffler's endomyocardial disease) is a type of RCM in which there is extensive endomyocardial fibrosis, often accompanied by an apical thrombus containing eosinophils. The fibrosis itself may be seen as a dark apical rim on gradient echo sequences.
Sarcoidosis involves the heart in about 25% of patients who have the disease. Sarcoid of the heart may appear as focal bright signal in the myocardium on T2 weighted images. Sarcoid granulomas typically demonstrate late hyperenhancement in a patchy midwall and epicardial distribution.
Amyloidosis involves the myocardium in nearly all cases of primary amyloidosis, but is less common in secondary amyloidosis. The imaging characteristics of cardiac amyloidosis include ventricular wall thickening and DHE. Amyloidosis typically demonstrates extensive midwall DHE. There may be thickening of the atrial septum or right atrial posterior wall as well.
Hemochromatosis can be either familial or acquired through multiple transfusions and is characterized by iron deposition in tissues throughout the body, including the heart. Iron deposition in the heart is predominantly subepicardial. Due to the paramagnetic nature of the iron deposits, signal loss is seen on both T1 and T2 weighted images. Iron deposit in the liver as well, resulting in an abnormally dark liver on MRI.

The cine on the top demonstrates poor diastolic relaxation and a mass in the LV apex. The image on the bottom is an image from a first pass gadolinium infusion which shows that the LV apex mass does not enhance (arrowhead). This patient has Loeffler's Endomyocardial Disease and the LV apex mass is a thrombus containing eosinophils.
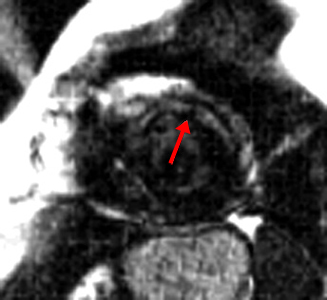
This image shows DHE in the anterior LV wall midwall (arrow) in a patient with sarcoidosis. This diagnosis is usually made by combining imaging findings with clinical suspicion. This imaging finding is nonspecific and could also be seen with amyloidosis or myocarditis.
![]()
![]()