PET/CT > Artifacts & Pitfalls > Elevated Glucose Level
Elevated Glucose Level
![]()

53 year old female with rectal adenocarcinoma metastatic to the liver status post low anterior resection followed by adjuvant chemotherapy. The patient also has poorly controlled insulin-dependent diabetes mellitus. PET/CT ordered for restaging.
The patient's serum glucose level at the time of FDG injection was 225 mg/dl. Although there was no definitely abnormal FDG activity evident on this examination, the study was interpreted as nondiagnostic due to the significant possibility of false-negative results in the setting of an elevated serum glucose level at the time of FDG injection. The interpreter recommended that the patient return for repeat examination to be performed only if the serum glucose level was less than or equal to 150 mg/dl. (In this case, the ordering physician actually decided to restage the patient with MRI. MRI showed no change in the size of several known liver metastases and no evidence of new metastases).
Elevated blood glucose levels create a potential problem in PET imaging. High levels of circulating glucose essentially "compete" with radioactive FDG for uptake in both abnormal (hypermetabolic) tissues (e.g. cancer or inflammation) and in normal tissues. This decreases the sensitivity for disease detection and therefore significantly increases the chance of obtaining a false negative result. For example, with a high serum glucose level although FDG activity in a lymph node involved by tumor may actually be greater in intensity than activity in normal tissues, activity in that lymph node may visibly appear relatively low-level and its SUV may be nondiagnostic for malignancy. This would constitute a false-negative result. In situations such as this, when patients have be re-examined under conditions of better glucose control, initially falsely-normal FDG levels have reverted to clearly abnormal levels in diseased tissues. Therefore, in order to decrease the chances of false-negative results as much as possible we have made a general policy that a PET/CT should not be performed if the serum glucose level is greater than 150 mg/dl. In the setting of a suboptimal glucose level on the scheduled day of an examination, the nuclear medicine physician should discuss the situation with the ordering physician so that he or she understands the reason for not performing the study and so that a plan can be made for rescheduling the examination under adequate glycemic control. Clear communication of these situations and the rationale results in benefit for both the patient and the ordering physician.
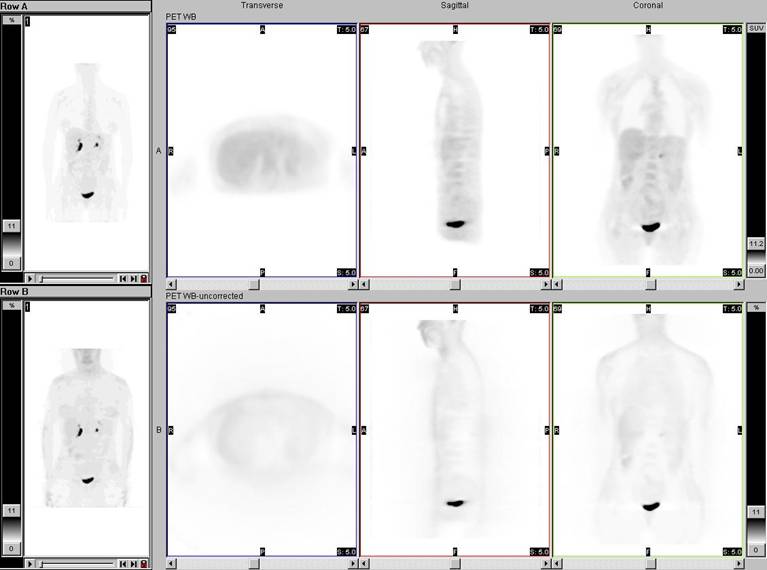
Attenuation-corrected and non-attenuation corrected data from the examination in the patient with elevated serum glucose level at the time of FDG injection described above. There is lower than usual intensity of FDG activity diffusely throughout the body. It is difficult to see any activity at all in some of the structures which normally demonstrate low-level FDG activity.
![]()
![]()