Emergency Ultrasound > Pelvic Pain > PID
Pelvic Pain - PID
![]()
Clinical
Pelvic inflammatory disease (PID) is caused by sexually transmitted infection, most commonly chlamydia or gonorrhea or both. PID also occurs as a complication of appendicitis, diverticulitis, pelvic abscess, and post-abortion or post-delivery infection. Acutely, patients present with fever, pelvic tenderness, and vaginal discharge. The inflammation commonly becomes chronic and patients present with pelvic mass and dyspareunia. Most cases occur in young, sexually active women, although 1-2% of tubo-ovarian abscesses are reported in postmenopausal women.
Transvaginal image of a normal ovary with surrouning follicles (red arrows).
Exam
Begin with the patient in the supine position.
Pelvic exam
Obtain longitudinal and transverse views of the bladder and longitudinal and transverse view of uterus (take measurement). Get longitudinal and transverse views of each ovary (take measurements). If torsion of the ovary is suspected, show color Doppler and spectral tracings of both venous and arterial flow.
ovarian mass > 2cm - Color Doppler and Doppler tracings with RI measurements.
View of each kidney when necessary (i.e. pelvic mass, ectopic pregnancy).
Endovaginal exam
Obtain sagittal and coronal views of uterus and each ovary.Measure both ovaries. Doppler and color Doppler all masses > 2cm.
Sonographic Findings:
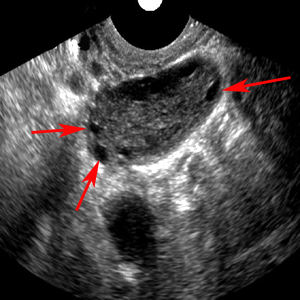
1) Pyosalpinx - pus-filled, dilated fallopian tube is recognized by the echogenic particulate matter that fills or layers within the tube.
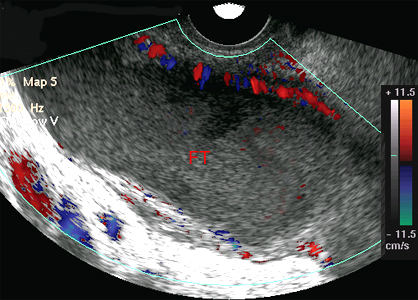
Transvaginal image of a dilated fallopian tube (FT) containing echogenic fluid.
2) Tubo-ovarian complex - dilated fallopian tube and inflamed ovary within a mass formed by adhesions. Pus appears as layering echogenic fluid and gas within mass.
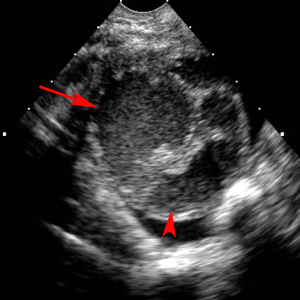
Tubo-Ovarian Complex. A markedly dilated fallopian tube (red arrow) partially envelopes the ovary (red arrowhead) in a patient with pelvic infection.
![]()
![]()