Emergency Ultrasound > Pelvic Pain > Ectopic Pregnancy
Pelvic Pain - Ectopic Pregnancy
![]()
Clinical
An ectopic pregnancy is implantation of a fertilized ovum outside of the fundus or body of the uterine cavity.Usually bleeding or pain in a patient with a positive BHCG is the common presentation. Ectopic pregnancy can never be excluded.We can confirm an intrauterine pregnancy (IUP) by documenting a yolk sac or a live embryo with a heartbeat.Ectopic pregnancy is much less likley if an IUP is found.
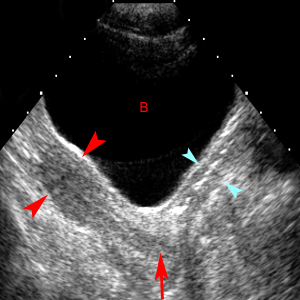
Longitudinal scan through the urine-filled bladder (B) demonstrates a normal adult uterus (red arrowheads) with smooth contours and pear shape. The cervix (red arrow) is recognized at the junction of imaginary lines drawn though the long axis of the uterus and the long axis of the vagina (blue arrowheads).
Exam
Start transabdominal and get whatever information you can. You may confirm an IUP and not need to do EV. If there is inadequate bladder distention or if you need to better visualize the uterine contents or ovaries, do EV. A female chaperon is mandatory.
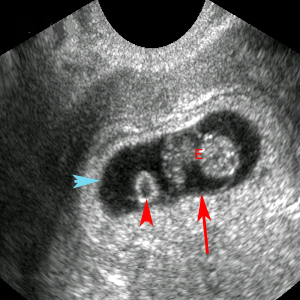
Transvaginal image of yolk sac (red arrowhead) and amniotic sac (red arrow). The embryo (E) is seen within the amniotic cavity. The chorion (blue arrowhead) is defined by the outer aspect.
Ultrasound Landmarks in Normal Pregnancy
|
Finding |
Expected Visualization |
Approximate Weeks |
|
Gestational sac |
BHCG > 1000 by EV; BHCG > 1800 by TA |
4.5 - 5 |
|
Yolk sac |
Mean sac diameter > 8 EV, > 18 TA |
5.5 - 6 |
|
Embryo |
Mean sac diameter > 16 EV, > 25 TA |
6 - 6.5 |
|
Fetal heartbeat |
Embryo > 5mm EV, any size TA |
6 - 6.5 |
BHCG:Normally doubles every one to two days. With ectopic pregnancy, the BHCG can increase (but less than would be expected for IUP), plateau or decrease. The BHCG decreases after spontaneous abortion unless there are retained products of conception. Serial BHCG measurements are very useful to distinguish between early IUP, spontaneous abortion and ectopic pregnancy. A follow up ultrasound can be obtained if the serial BHCG values are confusing.
Sonographic Findings:
1) Any abnormality outside the uterus significantly increases the risk of ectopic pregnancy.
2) Signs of an ectopic include adnexal masses, complex fluid, a ring of echogenic decidualized tissue involving the fallopian tube (tubal ring sign) or fluid in the cul-de-sac or Morrison's pouch.
3) An acute bleed may be very echogenic and blend in with the pelvic fat in the cul-de-sac and be missed unless you're specifically looking for it. Acute blood can also be anechoic.
4) An ectopic will often be on the side of the corpus luteum cyst but does not have to be.Beware of calling an ovarian follicle an ectopic; an ectopic always has an echogenic ring.
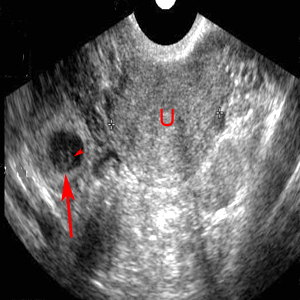
Transvaginal image of an extrauterine sac (red arrow) shows a tubal ring sign with thick echogenic wall and contains a yolk sac (red arrowhead). The presence of the yolk sac is diagnostic of extrauterine gestation. The U represents the uterus.

Transvaginal image of an extrauterine sac (red arrow) demonstrating the tubal ring sign adjacent to an ovary (red arrowhead). The tubal sign alone is less specific than a tubal sign with a yolk sac.

Transvaginal image of an empty uterus (U) with thickened endometrium (red arrow) representing decidual reaction in a patient with adenexal mass. Echogenic fluid (red arrowhead) is seen in the cul-de-sac. The combination of adnexal mass and echogenic cul-de-sac fluid makes this patient very high risk for ectopic pregnancy.

Transvaginal image of a cornual ectopic pregnancy (red arrow). The uterus is demonstrating a decidual reaction (red arrowhead).
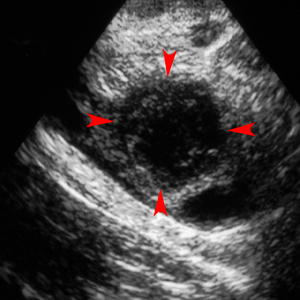
Thin-walled ovarian cyst containing anechoic fluid is likely the corpus luteum (red arrowheads) and is not predictive of ectopic pregnancy.
![]()
![]()