Modalities
of Liver Imaging

CT
|
- Uses X-ray to acquire data that can be
displayed in axial, coronal, and sagittal
planes.
- I.V. iodinated contrast is commonly used
in liver imaging to demonstrate any abnormal enhancement of a hepatic lesion
and to show vascular structures.
- An I.V. bolus of 100 to 150 ml of
iodinated contrast is often used. The contrast agent is injected into veins, travels to the heart, aorta, celiac trunk, hepatic arteries, liver parenchyma and mixes with blood in portal veins drained into venules and then hepatic veins and then out to the IVC.
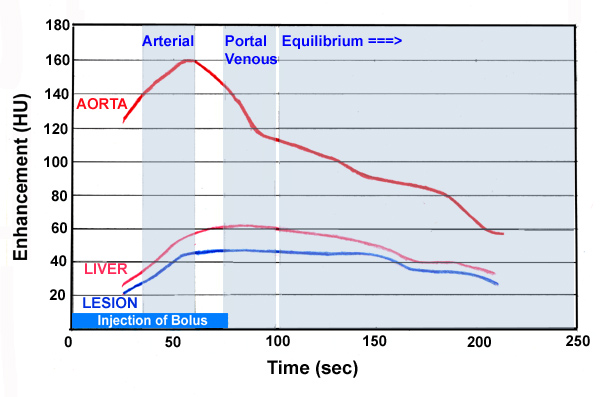
- Thanks to this temporal and spatial
disposition of the injected contrast agent, the hepatic enhancement can
be further divided into 3 phases: arterial phase (when the contrast just
fills up the aorta and the main hepatic arterial structures),
portal
venous phase (when the contrast disperses into the liver parenchyma and
mixes with portal blood), equilibrium phase (when the contrast further
scatters in the parenchyma and drains out the hepatic veins and also be
seen in the renal collecting system).
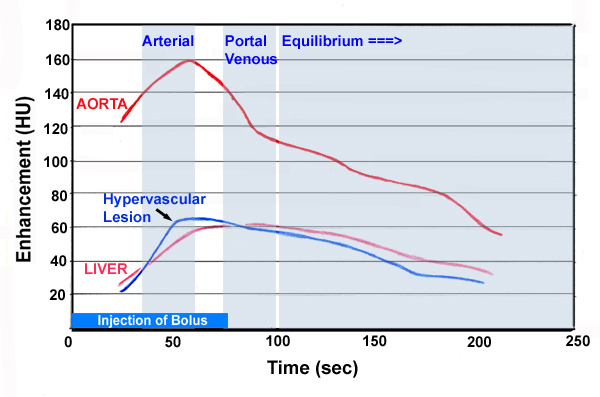
- When searching for hypervascular
lesions, such as hepatoma or metastastic disease, a three-phase
technique often should be used: non-contrast phase, arterial phase, and
portal venous phase.
- The appropriate delay times for scanning
in the arterial phase and portal venous phase for a 2-3 ml/sec injection
are 25 seconds and 70 seconds, respectively.
- The rationale behind this technique is
that primary and secondary malignancies of the liver typically have
hepatic arterial supply, thus will enhance during the arterial phase,
whereas benign entities and normal liver parenchyma have primarily
portal venous supply, therefore, will enhance during portal-venous phase
of I.V. contrast.
- The
liver parenchyma is normally homogeneous. Typically, the liver's
attenuation is 54-60 Hounsfield units (HU), usually 8-10 HU greater
than the spleen. Thus, the liver will appear hyperdense
to (brighter than) the spleen. If the density of the liver on CT is less
(darker) than that of the spleen, fatty change is most likely cause.
- The
vascular structures can be identified by their location on the
unenhanced images and confirmed by enhancement with intravenous
contrast. The intrahepatic biliary tree is not normally visualized
although the main right and left hepatic ducts are increasingly
demonstrated on modern systems and the common hepatic duct and common
bile duct are normally seen.
|
|

