|
Endocrine tumors include insulinomas, gastrinomas (Zollinger-Ellison
syndrome), glucagonomas, VIPomas (Verner-Morrison syndrome), and
somatostatinomas among others. While most insulinomas are benign, most
gastinomas, glucagonomas, VIPomas, and somatostatinomas are malignant.
Endocrine tumors of the pancreas are
occasionally associated with other syndromes, including von-Hippel-Lindau
disease (CNS hemangioma, renal cell carcinoma, adenomas and cysts of
liver/kidney/pancreas, and islet cell tumors, ), and multiple endocrine neoplasia
(MEN; pituitary, parathyroid, and pancreatic neoplasms).
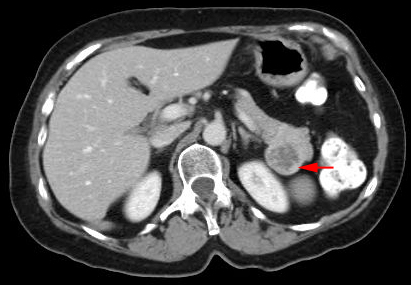
| Initial diagnosis of pancreatic endocrine tumors is based on
specific symptoms, followed by immunoassay detection of a particular
hormone. Imaging serves to localize the tumor. These tumors are less
difficult to diagnose because of their hypervascular nature. The tumors
appear as hyperdense masses on contrast-enhanced CT. Calcifications are
more frequently seen in islet cell tumors than in ductal adenocarcinoma. |
 |
Insulinoma:
Insulinomas are the most common islet cell tumors, and occur most frequently in females over 40 years of age.
More than 90% of insulinomas are benign. On US, inuslinomas appear as
hypoechoic masses which are well demarcated from surrounding
parenchyma. Most are smaller than 2 cm in diameter. EUS and
intraoperative US are most sensitive for localization. CT is also
highly accurate in the diagnosis of insulinomas. They appear as
hyperattentuating tumors. The optimal treatment of insulinomas is
surgical resection.
Gastrinoma:
Gastrinomas (Zollinger-Ellison syndrome) may be single or multiple;
60% are malignant. Most occur in men over 40 years of age. US and CT
have limited roles in the diagnosis of primary tumors because the tumors
are too small to be seen and may be ectopic. Ninety percent of
extrapancreatic tumors are in the "gastrinoma triangle." (This
"triangle" is bounded by the junction of the cystic and common bile duct
superiorly, the second and third portion of the duodenum inferiorly, and
the neck/body junction of the pancreas medially.) Barium studies and
endoscopy may show ulcerations in the stomach, duodenum and jejunum.
Octreotide scanning (somatostatin receptor scintigraphy) is commonly
used for diagnosis of gastrinomas. |