Chest Radiology > Pathology > Pneumothorax
Pneumothorax
![]()
A pneumothorax is defined as air inside the thoracic cavity but outside the lung. A spontaneous pneumothorax (PTX) is one that occurs without an obvious inciting incident. Some causes of spontaneous PTX are; idiopathic, asthma, COPD, pulmonary infection, neoplasm, Marfan's syndrome, and smoking cocaine. However, most pneumothoraces are iatrogenic and caused by a physician during surgery or central line placement. Trauma, such as a motor vehicle accident is another important cause. A tension PTX is a type of PTX in which air enters the pleural cavity and is trapped during expiration usually by some type of ball valve-like mechanism. This leads to a buildup of air increasing intrathoracic pressure. Eventually the pressure buildup is large enough to collapse the lung and shift the mediastinum away from the tension PTX. If it continues, it can compromise venous filling of the heart and even death.
On CXR, a PTX appears as air without lung markings in the least dependant part of the chest. Generally, the air is found peripheral to the white line of the pleura. In an upright film this is most likely seen in the apices. A PTX is best demonstrated by an expiration film. It can be difficult to see when the patient is in a supine position. In this position, air rises to the medial aspect of the lung and may be seen as a lucency along the mediastinum. It may also collect in the inferior sulci causing a deep sulcus sign.
A hydropneumothorax is both air and fluid in the pleural space. It is characterized by an air-fluid level on an upright or decubitus film in a patient with a pneumothorax. Some causes of a hydropneumothorax are trauma, thoracentesis, surgery, ruptured esophagus, and empyema.
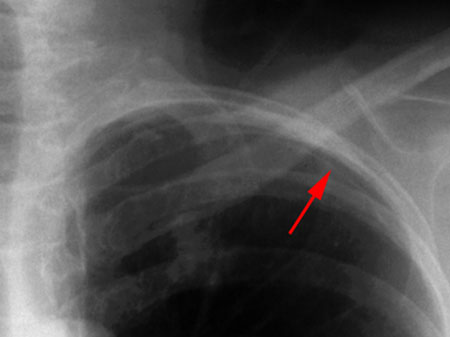
This image shows a close-up of a
pneumothorax in an upright PA exam as a white pleural line (red arrow) with
atmospheric air outside of it. No pulmonary vascular markings are seen
outside of the line. Notice the predilection to the apices and the periphery.
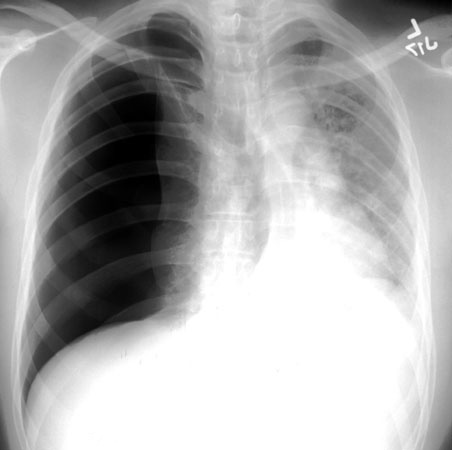
The above exam shows a right sided tension pneumothorax with
right sided lucency and leftward mediastinal shift. This is a medical
emergency. Failure to place a right chest tube immediately could allow
venous return to diminish and lead to possible death.
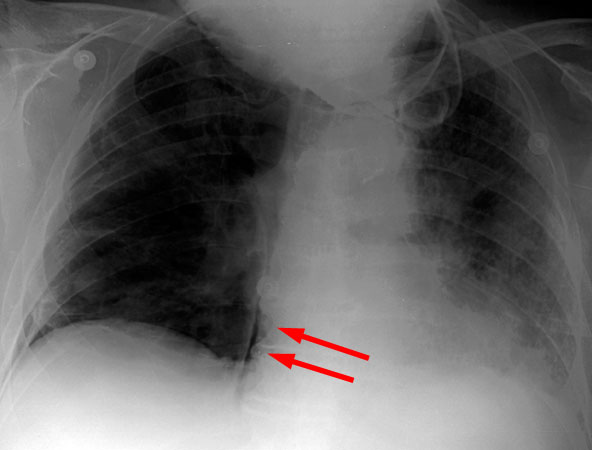
Left is a supine view of a PTX, note the medial position of
the air.
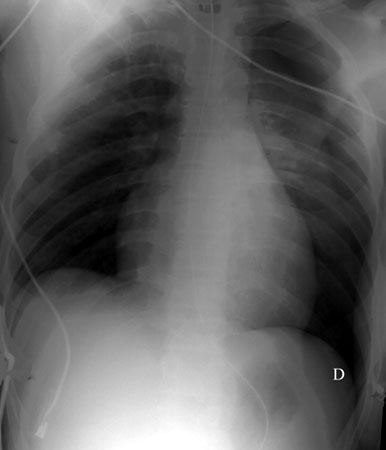
Right is an image demonstrating the deep sulcus sign (letter D in
the image) in supine views of a PTX.
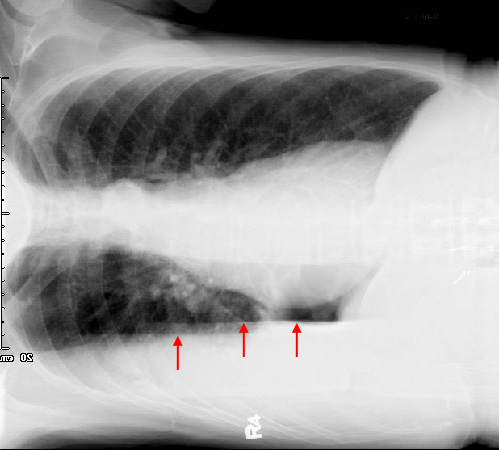

The above three images show a hydropneumothorax in three
different views.
The PA, lateral, and right decube reveal a layering out
of the air and fluid.
The right decube exam demonstrates a right hydropneumothorax.
Note the pleural air/fluid level demonstrated by the horizontal air/fluid
interface (arrows).
![]()
![]()
© Copyright Rector and Visitors of the University of Virginia 2013