Chest Radiology > Pathology > Atelectasis > Right Lung
Right Lung Atelectasis
![]()
Right Upper Lobe
Right upper lobe atelectasis is easily detected as the lobe migrates superomedially toward the apex and mediastinum. The minor fissure elevates and the inferior border of the collapsed lobe is a well demarcated curvilinear border arcing from the hilum towards the apex with inferior concavity. Due to reactive hyperaeration of the lower lobe, the lower lobe artery will often be displaced superiorly on a frontal view.
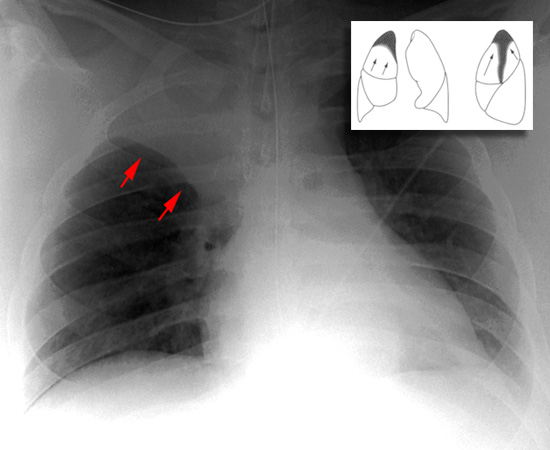
Note the elevation of the horizontal fissure (arrows) caused by RUL atelectasis.
Right Middle Lobe
Right middle lobe atelectasis may cause minimal changes on the frontal chest film. A loss of definition of the right heart border is the key finding. Right middle lobe collapse is usually more easily seen in the lateral view. The horizontal and lower portion of the major fissures start to approximate with increasing opacity leading to a wedge of opacity pointing to the hilum. Like other cases of atelectasis, this collapse may by confused with right middle lobe pneumonia.
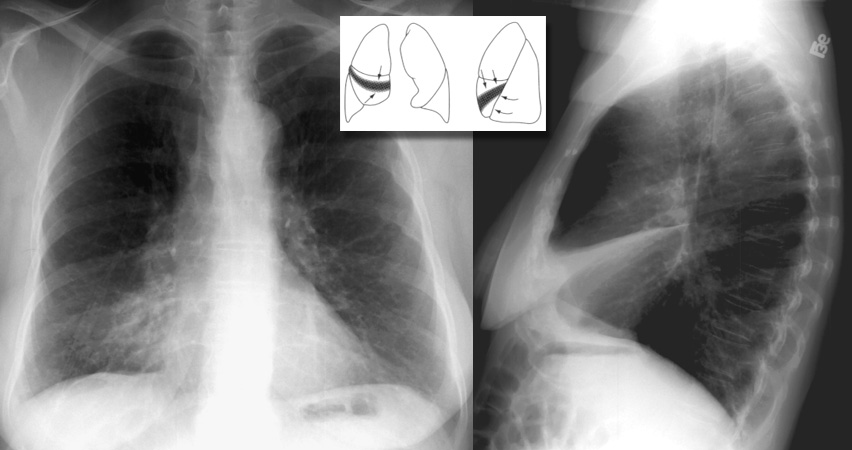
Right middle lobe atelectasis can be difficult to detect in the AP exam. The right heart border is indistinct on the AP exam. The lateral, though, shows a marked decrease in the distance between the horizontal and oblique fissures.
Right Lower Lobe
Silhouetting of the right hemidiaphragm and a triangular density posteromedially are common signs of right lower lobe atelectasis. Right lower lobe atelectasis can be distinguished from right middle lobe atelectasis by the persistance of the right heart border.
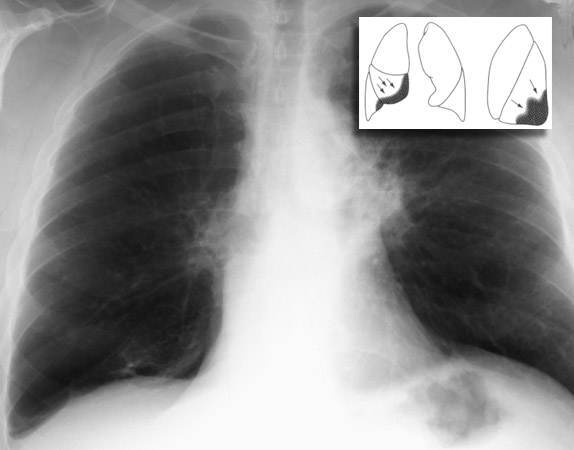
Notice the stretched vessels in the hyperexpanded right upper lobe in right lower lobe atelectasis. The right hilum is also displaced inferiorly. This is a tough one.
![]()
![]()
© Copyright Rector and Visitors of the University of Virginia 2013