Chest Radiology > Pathology > Pleural Effusion > Pleural Effusion
Pleural
Effusion
![]()
Common causes for a pleural effusion are CHF, infection (parapneumonic), trauma, PE, tumor, autoimmune disease, and renal failure.
On an upright film, an effusion will cause blunting on the lateral and if large enough, the posterior costophrenic sulci. Sometimes a depression of the involved diaphragm will occur. A large effusion can lead to a mediastinal shift away from the effusion and opacify the hemothorax. Approximately 200 ml of fluid are needed to detect an effusion in the frontal film vs. approximately 75ml for the lateral. Larger effusions, especially if unilateral, are more likely to be caused by malignancy than smaller ones.
In the supine film, an effusion will appear as a graded haze that is denser at the base. The vascular shadows can usually be seen through the effusion. An effusion in the supine view can veil the lung tissue, thicken fissure lines, and if large, cause a fluid cap over the apex. There may be no apparent blunting of the lateral costophrenic sulci.
A lateral decubitis film is helpful in confirming an effusion in a bedridden patient as the fluid will layer out on the affected side (unless the fluid is loculated). Today, ultrasound is also a key component in the diagnosis. Ultrasound is also used to guide diagnostic aspiration of small effusions.


PA and lateral exam of a patient with bilateral pleural effusions.
Note the concave menisci blunting both posterior costophrenic angles.
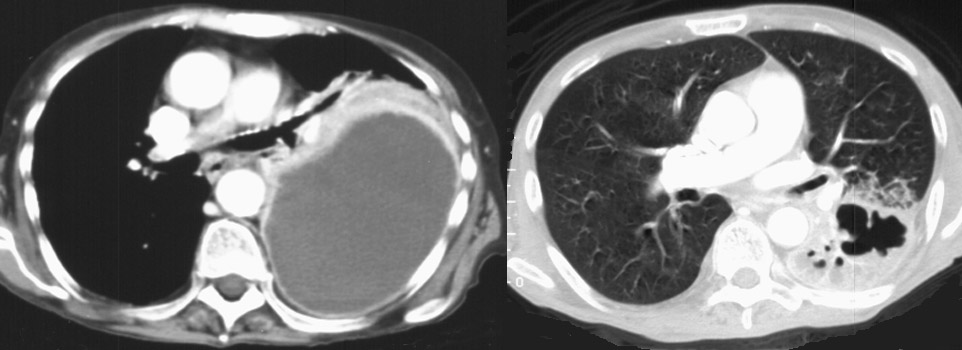
The CT above on the left demonstrates a large infected pleural fluid collection, an empyema. Compare and contrast that to the image on the right which is an intrapulmonary abscess.
![]()
![]()
© Copyright Rector and Visitors of the University of Virginia 2013